Introduction
Popular and effective cancer treatments, such as platinum-based chemotherapy agents, like cisplatin, and radiation may cause ototoxicity.1,2 Ototoxicity is the “functional impairment and cellular degeneration of the tissues in the ear caused by therapeutic agents, resulting in a loss of hearing and/or vestibular function”.3(p6) Details about the pathophysiology of ototoxicity caused by cancer treatments are discussed in detail by authors such as Landier.2 Ototoxicity may present as cochleotoxicity, vestibulotoxicity, or both.3 Cochleotoxicity may result in hearing loss that is either reversible or permanent and the degree of severity of hearing loss may vary.4–6 Hearing loss may also be accompanied by other auditory symptoms, such as tinnitus.4,6 Vestibulotoxicity may cause permanent bilateral vestibular hypofunction, which results in oscillopsia, gait ataxia, light-headedness, disequilibrium, and/or unsteadiness.3,7,8 Within the South African context of the quadruple burden of disease, agents used to treat diseases like TB and HIV/AIDS may be ototoxic, and the co-administration of these with cancer treatments that are ototoxic, may increase patients’ susceptibility to ototoxicity, and the ototoxic effects may be exacerbated.1 High dosages and long duration of cancer treatments, infusion rates and cumulative dosages, renal dysfunction, anaemia, age, and genetic predisposition, among other factors, may also increase the likelihood of ototoxicity, particularly cochleotoxicity.1,7,9,10 The incidence of ototoxicity caused by cancer treatments such as cisplatin is highly variable (0 to 100%) mostly owing to the aforementioned factors.11 However, a South African study that explored the incidence found that it was 55.1% and that South Africans seem to be at a higher risk for ototoxicity as compared to their South American and European counterparts.12
As a result of the auditory and vestibular dysfunction caused by ototoxicity, communication difficulties and/or vestibular difficulties are often experienced.13,14 Research indicates that cancer survivors deem speech hearing to be the largest hearing handicap.14,15 In addition, they also seem to experience difficulty with sound localisation, an auditory process that is necessary for group conversations.14,16 Due to these difficulties, participation in social events is restricted.12 People suffering from ototoxicity also report difficulty hearing in noisy environments and watching television.12–14 Cancer survivors who experience tinnitus report that communication is also impeded by this symptom, leaving them frustrated.14,17 These communication barriers affect familial relationships and result in survivors experiencing social anxiety and isolation.14
Cancer survivors with severe hearing loss and/or vestibular hypofunction caused by their treatment are reportedly dependant on others, particularly when needing to perform activities of daily living.7,14,17–19 They are also likely to be unemployed and their difficulties appear to affect their vocational aspirations negatively.7,18,19 According to Phillips,14 these effects may impact sufferers of ototoxicity from integrating successfully in their communities, resulting in their perceiving themselves as inactive members of society.
Moreover, ototoxicity reportedly results in high levels of stress and distress, particularly for those who experience tinnitus and/or vestibular difficulties.7,17,19 The psychological impact of ototoxicity may also be so intense among some cancer survivors that they may adopt suicidal mindsets.14 According to Phillips, in such instances, people have alluded to overdosing themselves, expressing that they would rather be dead than deaf.14,17
Children who are treated with cancer treatments that are ototoxic may experience speech-language and literacy delays when the period of treatment corresponds to the critical stage when hearing affects the development of those skills.20 Since speech and language acquisition relies on children receiving repeated verbal and auditory input, and they monitor their own speech through hearing, children being treated with cancer treatments that are ototoxic often present with speech sound errors and delayed vocabulary development when, for example, they miss out on this verbal input.21 Consequently, children’s scholastic performance is affected.13,14 Research into the academic and intellectual abilities of children acquiring hearing loss as a result of cancer treatment, has found that children with hearing loss displayed a significant decline in their academic and intellectual abilities.22 Similarly, adults who experience severe hearing loss as a result of their cancer treatment are also considered to be at risk for experiencing difficulties with language-related cognitive tasks, such as verbal reasoning, verbal fluency, and word reading.23 Other cognitive deficits may include difficulties with attention, processing speed, executive functioning, cognitive flexibility, and visuomotor speed.23 Similar to its impact on adults, parents of children receiving ototoxic cancer treatment reported that their children appeared to be miserable, frustrated, and anxious.14 Children were reportedly bullied, had difficulty making friends, and required support in social interactions.14
Although emphasis tends to be placed on reducing the burden of cancer through treatment to sustain life, from the above discussion it is evident that the effects of cancer treatment, like ototoxicity, and the psycho-socio-emotional, cognitive, occupational, and scholastic sequelae that they have can adversely affect quality of life.13,14 These effects may be accentuated in low- and middle-income countries, such as South Africa, due to limited audiological services.12 Ototoxicity can be prevented and the consequences of ototoxicity can be averted if the necessary audiological services are in place and operationalised effectively.13,24–28 Furthermore, including audiological services in cancer care will better aid South Africa in meeting the Sustainable Developmental Goal (SDG) Target 3.4, which relates to reducing the morbidity and mortality of non-communicable diseases through prevention and treatment, and promoting mental health and wellbeing.29
Methods
A review of literature was conducted to explore audiological service provision for cancer care in South Africa. The review focused on identifying the shortcomings and learnings of audiological service provision for persons receiving cancer care. It also aimed to highlight the initiatives and innovations to improve audiological service provision and access to quality care at a community level for cancer patients in South Africa. A wide variety of peer-reviewed publications and clinical guidelines that were relevant to addressing the aforementioned objectives were reviewed. The literature was sourced through PubMed, ScienceDirect, Google Scholar as well as the databases of the World Health Organization (WHO) and Health Professions Council of South Africa (HPCSA). Grey literature, such as a research report on the audiological service provision for cancer was also reviewed. A narrative approach was used. It enabled for the different types of literature to be synthesised and for the themes to be drawn across the data so that the objective of this review could be addressed.30 In addition, the shortfalls of the National Cancer Strategic Framework (NCSF) 2017-202231 were explored.
Findings
Current best practice: ototoxicity monitoring programmes and management
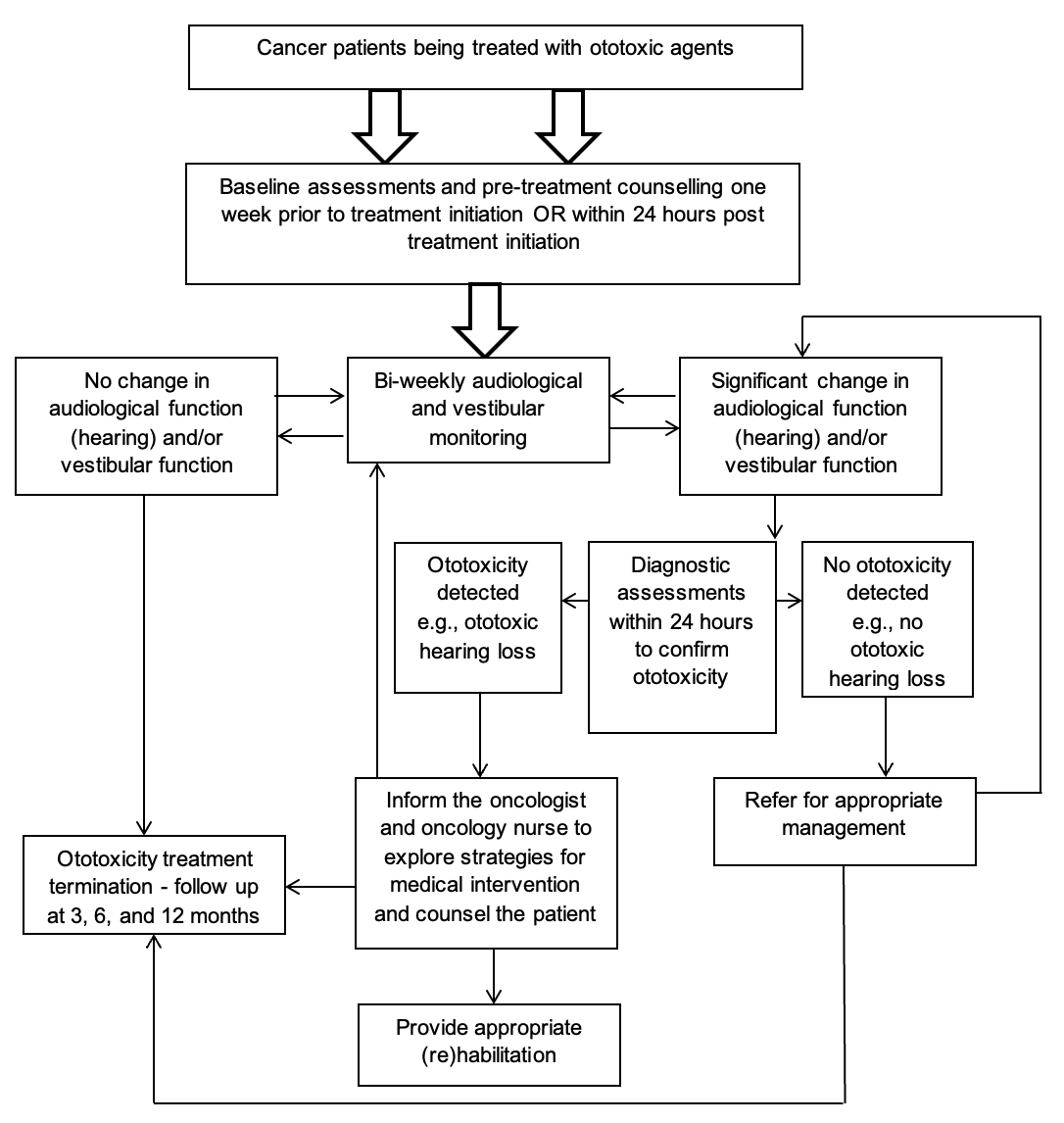
Ototoxicity monitoring is an audiological service or programme and a form of pharmacovigilance that must form part of the care of cancer patients who receive treatments that are ototoxic.6,13,24–28 The primary goal and ideal outcome of such a programme is to prevent hearing loss and/or vestibular dysfunction.13 For people who may not have benefitted from preventative opportunities, rehabilitation of auditory and/or vestibular dysfunction is the secondary goal and outcome.6,13 In 2018, the Speech, Language and Hearing professional board of the HPCSA published guidelines for ototoxicity monitoring.6 These guidelines are based on the international standards for ototoxicity monitoring.6,32,33 As indicated in Figure 1, an ototoxicity monitoring programme should identify patients being treated with ototoxic cancer agents, provide counselling for them on the potential effects of the treatment on the auditory and vestibular systems prior to initiating the treatment, conduct baseline audiological and vestibular assessments prior to commencing treatment, and perform a series of sequenced audiological and vestibular assessments at different intervals.6

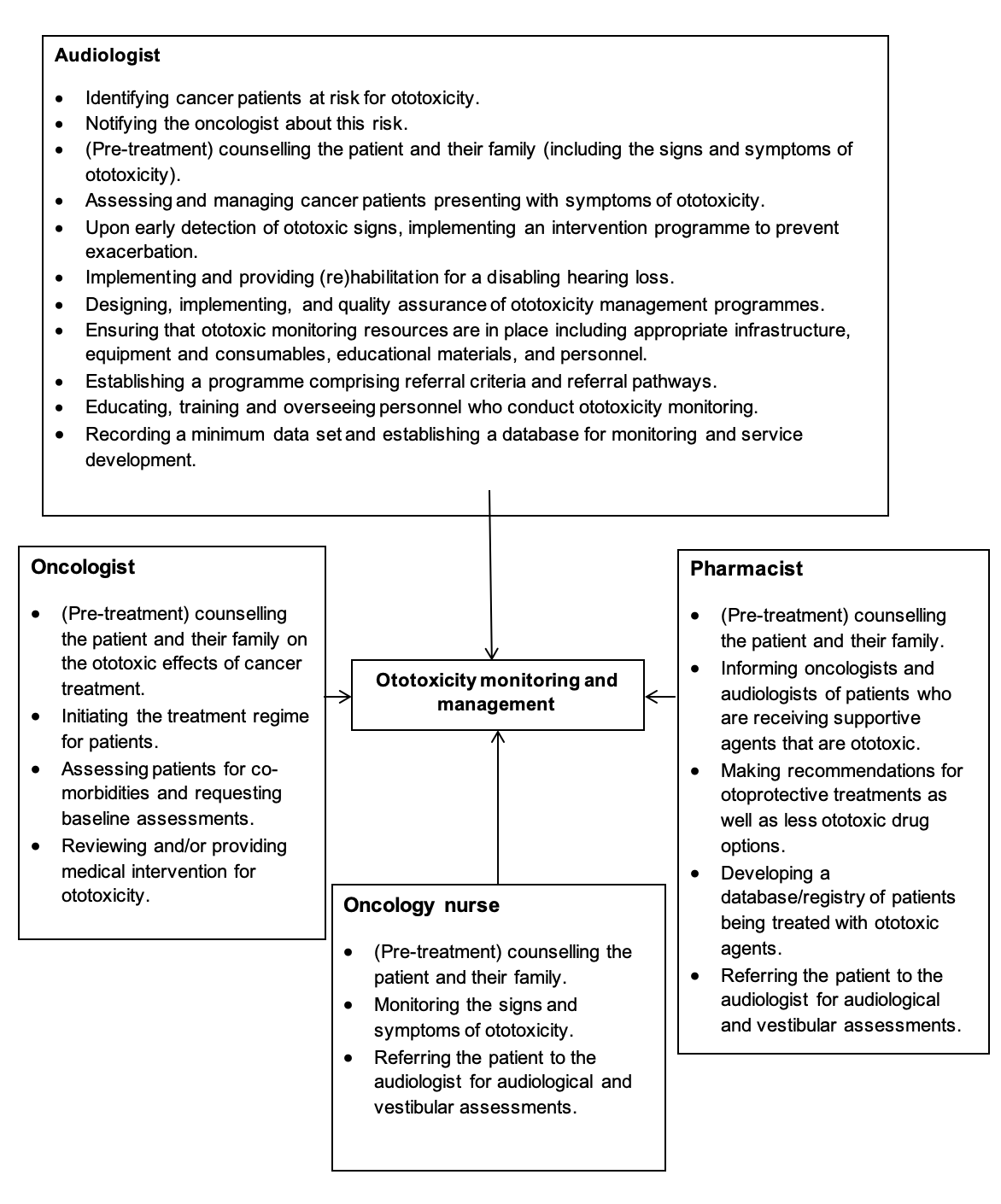
To ensure that the primary outcome of the programme is achieved, the ototoxicity monitoring programme needs to be facilitated by a multidisciplinary team (MDT).3,28 The MDT should comprise professionals involved in the management of cancer patients, including oncologists, oncology nurses, pharmacists, and audiologists.6,28,31 Other professionals who may form part of the MDT are social workers, clinical psychologists, ear, nose, and throat specialists, physiotherapists, occupational therapists, and speech-language therapists.6 Audiologists should drive the programme and patients should be at the centre of the programme.3,24,28
Current challenges and strategies to achieve best practice in audiological cancer care
In South Africa, the majority of the challenges surrounding implementing an effective ototoxicity monitoring programme seem to be logistical and resource related, e.g., staff shortages, lack of equipment, non-optimal testing conditions, and issues with appointment scheduling.13,24 The compromised physical health status of cancer patients also makes patients’ participation in audiological and vestibular assessments challenging to the extent that they may not be able to participate in the assessments.24 There are currently 39 audiologists per million people.34 This lack of capacity versus the demand for audiology human resources and the need for the equipment used in audiological and vestibular assessments further burdens the implementation of an effective ototoxicity monitoring programme.35,36 In the few instances where public health cancer facilities have attempted to ensure that patients receive audiological assessments, another cause of failure is the constant rotation of oncologists.24
Strategies such as lowering the cumulative doses of platinum-based chemotherapy agents that are ototoxic and/or prescribing less ototoxic agents, such as carboplatin instead of cisplatin, have shown to be effective in preventing or at least minimising the effects of ototoxicity if identified early.6,13,24 Recently, there has been promising evidence that otoprotective agents, such as D-methionine, may preserve auditory and vestibular function when co-administered with treatments that are ototoxic at the initiation of treatment.3,13 Currently, the use of neurotrophins to restore auditory-vestibular function and genetic screening to identify patients who are at higher risk of ototoxicity and for whom treatment with ototoxic agents may be contraindicated has gained much traction in research.3 Therefore, as some medications for vestibular dysfunction have been shown to potentially aggravate the symptoms of bilateral vestibular hypofunction, vestibular rehabilitation has been recommended to rehabilitate balance and gait issues.7 Furthermore, aural rehabilitation may be recommended, which could include the fitting of amplification devices, such as hearing aids or cochlear implants, and receiving communication training.6,13
Discussion
Need for a standardised ototoxicity monitoring protocol
Originally, there was no contextually relevant ototoxicity monitoring protocol and programme in place for cancer patients in South Africa.24,27,37 However, fair progress has been made in this regard, as reflected in the 2018 guidelines for ototoxicity monitoring and management published by the HPCSA,6 and it seems that currently, some sort of ototoxicity monitoring is conducted in South African cancer facilities.24 However, ototoxicity monitoring protocols sometimes deviate from the HPCSA guidelines when trying to accommodate unique circumstances, and may vary across contexts and cancer treatment protocols.24,38 Therefore, it would be remiss not to acknowledge the need for a national and standardised ototoxicity monitoring protocol.13,24,26 Notwithstanding this need, recent research efforts have provided insights to support best practice for ototoxicity monitoring protocols and programmes for cancer patients.5,24
Implementing practicable and effective assessments and monitoring
Ideally, audiological assessments should be conducted in sound-proof booths, but this may not be possible in many clinical environments, further hampering the effectiveness of ototoxicity monitoring.24,39 In addition, vestibular evoked myogenic potential (VEMP) testing, which is a sensitive evaluation of vestibulotoxicity, may not always be practical to perform and is time consuming.5 Cancer patients may have erratic treatment schedules and a myriad of consultations with other professionals, which can also make it difficult to adhere to the ototoxicity monitoring guidelines for audiological and vestibular monitoring assessments.24,39
Using tele-audiology,37,38,40 alongside task-shifting, may be an innovative and practical way to conduct ototoxicity monitoring and to ensure the effectiveness of the programme, as it circumvents the above-mentioned challenges.24,37,41,42 Mobile health (mHealth) tools, such as the smartphone audiometry ‘hearTest’ that is available in South Africa have shown to be an affordable, accessible, efficient, and effective means to deliver hearing health.24,41–43 The ‘hearTest’ tool allows for audiological assessments to be administered by trained paraprofessionals like community healthcare workers and in patients’ homes.43 The tool also has measures that are sensitive to detecting ototoxicity early.41 Should patients require professional audiological assessments, ‘hearTest’ is also able to link them to their nearest audiologist using geolocation.41
Initiatives, such as the WHO’s basic ear and hearing care resource,44 can be used to create awareness and to improve health literacy at a community level in terms of ear diseases and hearing loss,5 and can also be used to supplement smart audiometry. To complement this resource and the mHealth tool, WHO has also published a training manual45 that can be used to guide paraprofessionals and healthcare professionals working in primary health care practically to prevent, identify, and manage ototoxicity and ear disorders alike. Other recent and ongoing developments include the online publication of the Training in Assistive Products (TAP) modules, which can be used by community healthcare workers to acquire the necessary competencies to be able to provide devices like hearing aids, should cancer patients require this type of intervention.46
Similarly, ‘OtoCalc’, is a smartphone application developed in South Africa for detecting ototoxicity and its severity in patients with drug-resistant TB.47 ‘OtoCalc’ may also assist with monitoring the progression of hearing loss and may aid with the management of ototoxicity.47 This application also notifies healthcare professionals when patients start having communication difficulties and/or start experiencing psycho-socio-emotional effects caused by their hearing loss.47 It can be used by any of the professionals in the MDT, and can supplement the counselling provided to patients and their families.47 Since the patient data are stored in a centralised system, the data can be accessed by professionals at other institutions if the patient is transferred.47 ‘OtoCalc’ may also be used when conducting ototoxicity monitoring in cancer patients as the same principles and practices apply in detecting and managing ototoxicity in patients with drug-resistant TB to that of cancer patients.6 Using this application can therefore standardise and enhance the efficiency and sensitivity of an ototoxicity monitoring programme in detecting and managing hearing loss early in cancer patients being treated with ototoxic agents.48
In terms of monitoring vestibulotoxicity, recent research conducted in South Africa has shown that the video head impulse test (vHIT) is sensitive and specific to identifying vestibulotoxicity.5 It is a quick and objective test that can be performed easily in patients’ cancer treatment venues, thus overcoming the logistical challenges of conducting other objective vestibular assessments used in ototoxicity monitoring.5 In situations where tests like the vHIT are not available, then at least vestibular screening measures, such as dynamic visual acuity and head thrust should be used.5,7
Increasing awareness of ototoxicity
There appears to be an improved awareness and understanding among audiologists, oncologists, and pharmacists of the ototoxic effects of cancer treatment; however, it has been reported that oncology nurses have limited awareness regarding these effects.24,26,28,36,37 Research has reported that oncologists and oncology nurses do not seem to be aware of the factors that increase patients’ susceptibility to ototoxicity and thus do not enquire of their patients about them but limit their inquiry to the causes and associated conditions of cancer.28,37 This lack of awareness and limited inquiry may increase the risk of not identifying ototoxicity, which consequently reduces early identification and management of the problem. Not identifying patients at risk for ototoxicity may also explain why patients are not referred for baseline assessments.28,37 Patients tend only to be referred when they complain about a decline in their hearing sensitivity, and then oncology nurses often refer these patients to ear, nose, and throat specialists as opposed to audiologists.28 Referring patients to the incorrect professional may delay management, compromise the quality of care, and impose unnecessary costs for patients and the healthcare system.48 It also seems that, in the private sector, patients refer themselves to audiologists, and do so only once they experience a decline in their hearing sensitivity.24
Defining roles and responsibilities of the MDT
Despite improvements among the majority of members of the MDT, there seems to be uncertainty and unfamiliarity among professionals who form part of the MDT regarding their and each other’s roles in terms of ototoxicity monitoring and management.28 Arising from this ambiguity about roles and responsibilities, patients are often not informed of the ototoxic effects of cancer treatments during pre-treatment counselling.28 This, in turn, can impede early identification and intervention of hearing loss.24,28,36,37 It also compromises the ethical values of good practice as set out by the HPCSA49 and takes away from providing patient-centred care because patients may not be able to make informed decisions regarding their treatment.28
Generally, in terms of the management of ototoxicity, audiologists share information about patients’ audiological and vestibular function with the oncologists so that they may consider adjusting dosages, administrating otoprotective agents, and/or prescribing less ototoxic medication.24 However, it seems as though audiologists’ input is not always considered in this regard,24,26 which may increase the risk of ototoxicity that otherwise could have been prevented. These ototoxic sequalae may then necessitate audiological rehabilitation, such as the need for assistive technology in the form of hearing aids.13 It is probable that this lack of collaboration may be due to the widely accepted utilitarian, consequentialist, yet impartial view that sustaining life and the psycho-socio-emotional and financial consequences associated with cancer supersede the psycho-socio-emotional and financial consequences of ototoxicity caused by cancer treatments.24,50,51
Recommendations
Collaborative work to foster holistic practice in audiological cancer care
Effective communication and collaboration are needed through discussion forums and MDT meetings.28,39 Clear definitions of the roles and responsibilities of the MDT professionals are required, as indicated in Figure 2. Furthermore, awareness campaigns and continuous professional education may engender awareness and knowledge on topics like the risk factors of ototoxicity in cancer patients, strengthen knowledge and understanding of ototoxicity and ototoxicity monitoring, and enhance the involvement of professionals in ototoxicity monitoring.24,28,37 In addition, not having a centralised and automated database from which patients at risk for ototoxicity can be identified may account for the logistical reasons that hinder referrals for audiological and vestibular assessments.28,52 The aforementioned initiatives may facilitate early detection and intervention of ototoxicity.

Increasing recognition of the burden of cancer treatments in future iterations of the NCSF
Because of the emphasis and priority given to cancer survivorship and potentially life-saving treatment, as well as the adverse effects of cancer treatment such as nausea, vomiting, dehydration, and persistent weakness, hearing and vestibular difficulties tend to be underappreciated.5,24 The NCSF 2017-202231 acknowledges the morbidity of cancer and makes reference to quality of life but does not place sufficient emphasis on the morbidity associated with cancer treatments, such as ototoxicity and its effects. Therefore, in the development of the next NCSF, there is a need to account for this morbidity and to provide explicit measures and initiatives to prevent and control it. This development may strengthen the NCSF’s aims to mitigate the burdens of cancer placed on South Africans and to ease their distress and suffering. It will also make the framework more holistic and, therefore, should better guide cancer care so as to minimise the severe morbidity experienced by some cancer survivors. Through future versions of the NCSF and other related frameworks spotlighting the effects of cancer treatments, like ototoxicity, emphasis can be placed not only on survivorship but also on the quality of life. Even cancer patients nearing the end of life prefer and emphasise the desire to have quality of life over aggressive treatment that may extend their life.53
Conclusion
Commonly used cancer treatments of the priority cancers are ototoxic.1,2 Ototoxicity has dire consequences on quality of life and is burdensome, even more so in South Africa, where audiological services are limited.12–14 Ototoxicity, which is preventable,13 adds to the severe morbidity experienced by cancer survivors if not identified and managed early. This review has shown that an ototoxicity monitoring programme could allow for ototoxicity and its effects to be identified and managed early on so as to prevent or minimise the associated ramifications. The integration of innovative and practical strategies, such as mHealth tools and awareness campaigns, which are in line with technological advancements and collaborative work, such as providing ototoxicity monitoring in an MDT, would enhance current ototoxicity monitoring programmes. Future research should explore the achievability of employing these strategies for ototoxicity monitoring in cancer care in South Africa. Furthermore, research ought to be conducted focussing on rehabilitation options and opportunities. This paper provides a narrative review perspective; it is therefore recommended that for future research, other perspectives, such as a systematic review, as well as empirical research should be explored to build on knowledge regarding audiological service provision for cancer care in South Africa.
Future iterations of the NCSF should place equal emphasis on the burdens of cancer treatment as it does on cancer. This emphasis would support ototoxicity monitoring for cancer patients who are treated with ototoxic agents, and would thus better aid South Africa in meeting the SDG Target 3.4. The inclusion of audiological services as a core standard for cancer patients receiving ototoxic treatment may strengthen cancer care and allow for comprehensive, holistic, patient-centred best practice that is contextually attuned.