Background
Although all governments and multilateral health organisations, such as the World Health Organization (WHO), had already identified the threat posed by novel zoonotic diseases and had previously faced pandemics such as the 2009 influenza outbreak, the novel coronavirus that spread globally in early 2020 posed fresh challenges. The virus, quickly named SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), was identified as the cause of the novel COVID-19 disease. The virus was spread via the respiratory route, although early on there was considerable uncertainty about the role of droplets versus aerosols. How best to respond at a population level was therefore deeply contested from the outset. Greenhalgh et al. documented how the competing narratives (“about problems, how they arose, and how they will be resolved”) shaped advice and policy-making on COVID-19 in the United Kingdom.1 Such decisions are intrinsically ethical in nature, and not merely scientific.2
In South Africa, the national government reacted swiftly to the first imported cases and the evidence of local spread, invoking the Disaster Management Act (57 of 2002)3 on 16 March 2020.4 The Minister of Co-operative Governance and Traditional Affairs (COGTA) cited the “magnitude and severity of the COVID-19 outbreak”, the fact that it had been declared a global pandemic by the WHO, and that it had been “classified as a national disaster by the Head of the National Disaster Management Centre”, as justification for that step. The declaration was followed by a plethora of regulations, issued in terms of the Disaster Management Act, over the next two weeks. The regulations imposing significant restrictions on the populace were issued on 18 March 2020.5 These regulations authorised the Minister of Health to “issue directions to address, prevent and combat the spread of COVID-19 in any area of the Republic of South Africa”. The national ‘lockdown’ was instituted on 26 March 2020.
Directives (also referred to as directions) were also issued by various Ministers, all relying on the enabling provisions of the same Act. To cite just one example, a directive issued on 26 March 2020 by the Minister of Transport covered “improved access and hygiene, disinfection control on all public transport facilities”.6 The directive required the provision of “adequate sanitizers or other hygiene dispensers for washing of hands and disinfection equipment for users of public transport services”. All vehicles were to be “sanitized before picking up and after dropping off passengers”, all drivers were to wear masks, and all minibuses had to reduce their seating capacity by 50%. These directives, issued within 10 days of the declaration of the state of disaster, were based on the understanding of risk factors for COVID-19, and assumptions about droplet transmission and therefore the role of fomites. In a time of considerable uncertainty, the South African government needed to take rational and justifiable policy decisions backed by the available scientific evidence, which in the earlier stages of the pandemic was sometimes scanty. How and where to ensure access to the best scientific advice was never simple.
As governments across the globe responded to the rapidly developing COVID-19 pandemic in 2020, many were at pains to portray their decisions as being backed by scientific evidence, and therefore as being both rational and justifiable. In some countries, that advice was personified by a leading scientific voice, such as Dr Anthony Fauci in the USA. Heads of State would make policy announcements flanked by scientific and medical advisors. Despite such implied backing, an assessment of the policy-making process in four European countries (Germany, Italy, the Netherlands and the UK) by Hodges et al. noted “a growing gap between scientific advice and political decisions”.7 The authors of that paper argued that “advisors followed not only their particular logics as scientists, but were also receptive to the broader politically-centred logics of their clients, such that the boundaries between scientific advice and political decision-making became blurred”. In particular, they noted that “[e]xperts appointed by the Italian Government rarely released opinions conflicting with government decisions”. Greenhalgh et al. have argued that “UK policy makers seemed to favour narratives from a narrow group of scientific advisers”.1 As a result, it has been suggested that transparency and autonomy are key to ensuring that “governments do not simply seek advice that aligns with what they want to hear”.
Approach
This chapter reflects on the process of preparing advisories, the development of rapid evidence syntheses and their use in decision-making, the outputs and the lessons learned from that process, and the structural and operational changes over the course of the pandemic. The focus is exclusively on the Ministerial Advisory Committee (MAC) on COVID-19, which was established in March 2020 and that evolved both as a structure and in its outputs over the period to date. The chapter was authored by a writing group made up of members of the MAC and charged with this responsibility by the MAC on COVID-19. The writing group relied on reflection and discussion of available documentation and processes. The text of the chapter was circulated to all current MAC members for comment. Hence this chapter represents the perspective of the current MAC on COVID-19. In anticipation of a close-out report, the MAC on COVID-19 developed a reflection document, which informed this perspective. Periodic update reports were also available for reference.
Discussion
The processes followed, the changes made over time, and the lessons learned on reflection are outlined below.
Multiple structures
The Disaster Management Act established a number of structures intended to enable co-ordinated, government-wide responses to a declared disaster. The Intergovernmental Committee on Disaster Management, as established by the Act, included the Minister of COGTA, Members of the Executive Councils (MECs) from the provinces, and members of municipal councils, selected by the South African Local Government Association (SALGA). The National Disaster Management Centre, located within the responsible national department, is supposed to be backed by a National Disaster Management Advisory Forum, drawing on a wide range of constituencies, including “medical, paramedical and hospital organisations”. However, it quickly became apparent that a different co-ordinating structure had been created, termed the National Coronavirus Command Council (NCCC), supported by the National Joint Operational and Intelligence Structure (NatJoints).8 The NCCC was chaired by the President and included selected members of the Cabinet (including the Minister of Health). The President’s Coordinating Council (PCC) was also engaged at times; this Council comprised of the President, premiers of the provinces, executive mayors of metropolitan municipalities and the leadership of SALGA. The advisory structures established by the Minister of Health need to be viewed against this background of multiple overlapping structures. Crucially, management of the pandemic response was not primarily in the hands of the Ministry of Health, but in the hands of the Minister of COGTA.
The Ministerial Advisory Committee on COVID-19 – shifting compositions
Section 91 of the National Health Act (61 of 2003) enables the Minister of Health to appoint advisory and technical committees, after consultation with the National Health Council.9 By notice in the Government Gazette, the Minister may designate the “composition, functions and working procedure” for such committees.
Accordingly, the Minister of Health established a Ministerial Advisory Committee (MAC) on COVID-19 in March 2020. This initial MAC was composed of 51 members, but operated through four sub-committees, focusing on clinical care, public health, laboratory investigation, and research. The MAC included members with expertise in a wide range of areas, including infectious diseases, intensive care, paediatrics, laboratory services and diagnostics, vaccines and therapeutics, medicines regulation, disease modelling, implementation science, social science and research. The initial MAC was chaired by Professor Salim Abdool Karim. In October 2020, the MAC was reduced to 21 members, and Professor Marian Jacobs was appointed as a co-chair. In March 2021, following the resignation of Professor Abdool Karim and five other members, Professor Koleka Mlisana was appointed as a co-chair. Although five additional members were appointed, two further resignations brought the total number of members to 19. No payment was offered to any MAC members.
The focus of this chapter is on the MAC on COVID-19 from inception, but more particularly, the lessons learned and changes made after March 2021. After the establishment of the MAC on COVID-19, three additional MACs were also established: the MAC on COVID-19 vaccines (VMAC), the MAC on Social and Behavioural Change (both established in August 2020), and a MAC on COVID-19 Therapeutics (established in July 2021, replacing a sub-committee of the National Essential Medicines List Committee (NEMLC)). The MAC on COVID-19, while enjoying a wide remit, was not arranged hierarchically in relation to the other MACs. Some co-ordination was, however, enabled through cross-membership, and through engagement at the level of the National Department of Health (NDoH) Incident Management Team (IMT), which met on a weekly basis. In a limited number of instances, cross-MAC advisories were developed, issued jointly by two structures. Examples included the advisory on addressing vaccine hesitancy and the advisory on vaccination of children aged 5 to 11 years.10,11 The processes followed by the NEML MAC on COVID-19 Therapeutics have been reported elsewhere.12,13
Challenges faced by the MAC on COVID-19
As with any structure that is newly formed to respond to an emergency, perfect planning is not always possible, and for this reason lessons must be learned for future pandemic responses. The MAC on COVID-19 was no exception, and there were several challenges along the way. Soon after the establishment of the MAC on COVID-19, some MAC members were interviewed by a national news outlet where they shared their varying views on the effectiveness or otherwise of the lockdown to date. Although some were of the opinion that MAC members should not be voicing views critical of government policy, this had to be balanced against the right of MAC members, many of whom were academics, to express their personal views. Several MAC members resigned as a result of this controversy, which caused some discomfort among the newly constituted MAC membership. In August 2021 the Minister of Health, Dr Mkhize, was asked to stand down by the President. He was succeeded by Dr Phaahla. As a medical practitioner and previous Deputy Minister of Health, Dr Phaahla was able to ensure continuity and to request advice from the MAC on COVID-19 as before. It is important that any emergency structures should be constituted in a way that is resilient should unexpected external political changes occur.
The terms of reference of the MAC on COVID-19
The terms of reference of the MAC on COVID-19 changed over time to accommodate different ways of working and to reflect the changes in composition and the creation of additional MACs. Box 1 shows the remit of the MAC from June 2021, as stated in its terms of reference.14 Critically, while the MAC was expected to provide advice on the request of the Minister, Director-General of Health or the NDoH, it was also enabled to initiate advisories without such a request.
The terms of reference of the MAC on COVID-19 emphasised that “Members of the MAC are participants in their individual capacity and do not represent any constituency, organization or sector”. The rights of MAC members were also protected, as follows: “MAC on Covid-19 members are not prohibited from media communication in their personal capacity. However, under no circumstances may a committee member, other than the Co-Chairpersons of the MAC on Covid-19, officially represent the views and decisions of MAC on Covid-19 in the media or anywhere else in the public domain. Committee members approached by the media or anyone else for information on the MAC, its views and its advisories should direct these requests to the Secretariat.” Further, it was stated that “While Committee members are free to voice their personal views on any matter in public or in the media, they are requested to preferably refrain from commenting on matters under active deliberation by the committee. Once the deliberations on a matter have been completed and an Advisory submitted, then committee members should feel free to voice their personal views regardless of whether these personal views concur or differ with the advice provided by the MAC on Covid-19 in its Advisories.” The terms of reference also stated that “MAC on Covid-19 advisories and associated documents will be published at the discretion of the Minister of Health on the following website: https://sacoronavirus.co.za/category/mac-advisories/”, although no timeline for publication was specified.
The process used to develop an advisory
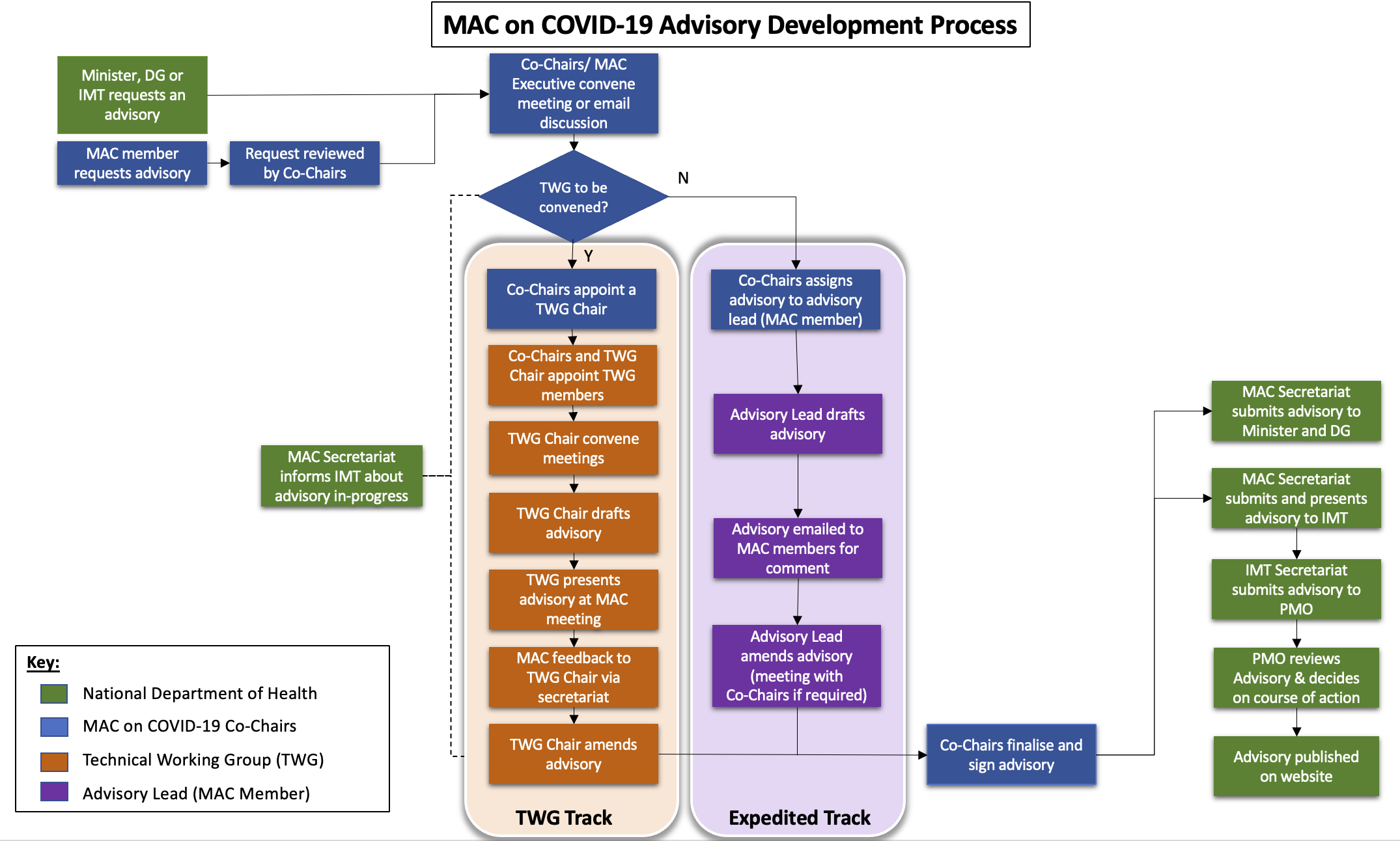
By accessing the best available scientific evidence, and then bringing the collective experience of its members to bear, the MAC on COVID-19 aimed to offer clear and actionable advice to the Minister of Health. Figure 1 shows the process of developing an advisory as it eventually operated in the final iteration of the MAC on COVID-19.
__209968_.png)
Whether in response to a request or on their own initiative, the MAC was expected to provide technical guidance that was context-specific and based on the best available evidence, locally and internationally, drawing on the systems-wide, multidisciplinary experience of its members. In addition, the MAC was able to constitute technical working groups (TWGs) by including members from outside of the MAC. An expedited track was also enabled, drawing on selected MAC members, with an opportunity for rapid review by the full MAC prior to submission of an advisory that required a short deadline.
Membership of the MAC also enabled linkages with critical scientific and regulatory structures, including the National Institute of Communicable Diseases (NICD), the Burden of Disease Research Unit at the South African Medical Research Council (SAMRC), the South African COVID-19 Modelling Consortium (SACMC), the Network for Genomic Surveillance in South Africa (NGS-SA), the South African Health Products Regulatory Authority (SAHPRA), and the WHO. However, where members of the MAC on COVID-19 also served on other MACs, on regulatory advisory and governance bodies, or on WHO structures, these involvements also had to be managed as potential conflicts of interest, with due regard to confidentiality requirements imposed by such bodies.
Input documents and data that were reviewed regularly included reports from the IMT, the NICD (including hospital admission and death data from daily hospital surveillance (DATCOV)), SACMC projections, NGS-SA reports, and SAMRC excess death estimates. A broader range of sources could be cited in support of advisories, as gathered and assessed by the TWGs and MAC members.
The least well-described portion of the process in this flow chart is that dealing with the actions taken by the Project Management Office (PMO) in the NDoH, in response to the advice received. In addition, the role of the Minister, as the ultimate recipient of the advice, is not stated. As indicated above, the range of actors that could possibly be involved in taking such decisions was extensive, and involved both other government departments and executive structures, such as the NCCC, Natjoints and the PCC. The timing of such decision-making could also be highly variable, depending on the complexity of the issue and the number of potential actors involved. The process by which a MAC advisory was used to guide government decision making in departments other than in health remains unclear. Advisories that touched on aspects primarily managed by other government departments, such as the Department of Basic Education and the newly-created Border Management Authority, were more difficult to link. One of the last advisories issued by the MAC, regarding the appropriate response to the Omicron outbreak in China, is perhaps most obviously linked to the action subsequently taken.15 The MAC’s recommendation not to impose restrictions on travellers from China was accepted.
Figure 1 also does not do justice to the critical role of the secretariat. Secretariat functions for all of the MACs were provided by pharmaceutical policy specialists from the Affordable Medicines Directorate at the NDoH, with support from external donor-funded technical advisors already in place within that unit. Their inputs were crucial to the successful development of advisory documents, the functioning of TWGs and the MAC, and the co-ordination with the IMT and PMO. With the exception of one weekend face-to-face workshop in February 2022, all TWG and MAC deliberations were held virtually, and decisions were taken in virtual meetings or via email.
The last step depicted in Figure 1 refers to publication of the advisory on the website. On recommendation from the MAC on COVID-19, the Director-General agreed in March 2022 to publish all advisories within seven days from receipt by the Minister of Health. The MAC believed that the timely availability and accessibility of the submitted advisories to the general public potentially enhanced public trust. In this way, the public could be informed of the scientific opinion expressed, providing important context for the political decisions that were subsequently taken, whether or not those aligned with the advisory’s recommendations. As Jarman et al. put it: “Advising is not decision making. Good advice systems preserve the autonomy and credibility of the advisers and scientists by separating their advice from actual decisions.”16 Although the MAC is not directly listed as a respondent, the issue of transparency is central to the court challenge brought by Sakeliga, which questioned the process for declaring a state of disaster.17 The experience of the MAC on COVID-19 in this regard should inform future best practice on information sharing with the public. Nonetheless, it should be anticipated that in an emergency some decisions will not go according to plan and will be open to challenge. Transparency in responding to problems and criticisms is critical to retaining public trust.
Advisory outputs
From its inception in March 2020 to July 2022, the MAC on COVID-19 produced 154 advisory documents. Initially, some were in the form of memoranda or responses to a particular narrow request. The first memorandum dealt with the wearing of cloth masks by the public. Early memoranda and advisories also covered direct clinical care questions, such as the options for respiratory support and the evidence for and against specific medicines, such as dexamethasone and ivermectin. Advisories also addressed such contentious issues as the use of disinfection tunnels, reliance on serological testing, self-testing using rapid antigen tests, school attendance, and controls at points of entry into the Republic. Not unexpectedly, it is difficult to track each piece of advice to a final decision, let alone to its effective implementation and the outcomes that resulted. In addition, some initiatives were decided upon at a political level without MAC consultation, such as the prohibition on selling tobacco products.
Only 113 of the 154 advisories provided by the MAC on COVID-19 were eventually published on the dedicated website. A separate website was created for the MAC on COVID-19 Vaccines (https://sacoronavirus.co.za/category/mac-advisories-vaccinations/) but not all earlier advisories were shared on this platform. The NEML MAC on COVID-19 Therapeutics also placed their rapid reviews in the public domain (http://www.health.gov.za/covid-19-rapid-reviews/). Members of this MAC also evaluated controversial subjects, such as the role of ivermectin in preventing and treating COVID-19.18 However, no publicly accessible repository of advisories from the MAC on Social Behaviour Change was developed.
The MAC’s role in critiquing the appropriateness of South Africa’s legislation
In addition to public health and clinical issues, the MAC also produced an autonomous advisory that identified key legislative tasks requiring attention.19 In this advisory, the MAC noted that South Africa’s International Health Regulation Act (28 of 1974) predated the current global legislation called the International Health Regulations (2005).20 This global legislation allows the WHO to make temporary recommendations that are binding on member states in the event of a global public health emergency. The South African 1974 Act is not well aligned with this global legislation, and has limited Regulations issued most recently in 2003.21 A draft Bill to address this deficiency was published in 2013, but never tabled.22 The MAC also noted the lack of progress in implementing the National Public Health Institute of South Africa (NAPHISA) Act (1 of 2020).23 Lastly, the MAC expressed its misgivings regarding the proposed regulations on notifiable medical conditions, issued for comment in terms of the National Health Act.24 The comment period on these regulations has been extended, but revised versions have yet to be published, either for further comment or in final form.
Global experiences
The Lancet COVID-19 Commission published an extensive report and recommendations in October 2022.25 At a national level, they characterised the strengthened health systems elements that were needed as follows: “strong relationships with local communities and community organisations; surveillance and reporting systems; robust medical supply chains; health-promoting building design and operation strategies; investments in research in behavioural and social sciences to develop and implement more effective interventions; promotion of prosocial behaviours; strong health education for health promotion, disease prevention, and emergency preparedness; effective health communication strategies; active efforts to address public health disinformation on social media; and continuously updated evidence syntheses”. The last of these speaks directly to the need to institutionalise the capacity to continuously update the evidence to inform public policy. Other demands speak to the need for improved transparency and proactive communication to improve public trust and counter disinformation.
In some countries, there have been urgent calls for the establishment of official inquiries into the manner in which the pandemic was managed in their national settings. For example, the questions raised about the way in which UK scientific advice was elicited and used include: “why did it take so long to increase the transparency of SAGE and other government scientific advice bodies; where, if anywhere, did government get advice about trade-offs and broader policy implications of public health measures; why do UK science advisers have so little autonomy from the government?”15 Hodges et al. characterise the context in which advice was provided as one of “conflicting values under substantial uncertainty about options for actions”.7 The question that has to be asked is how that uncertainty can be reduced, but also how the provision of high-quality, independent advice can best be institutionalised. The latter is not as contradictory as it may appear at first glance. Hodges et al. further argue that, in the four countries they surveyed, political responses to scientific advice varied, as the pandemic progressed: “In early stages, immense uncertainties about the effectiveness of potential interventions for fighting the outbreak and spread of the virus induced leading politicians to rely heavily on medical expertise for justifying severe constraints on the lives of citizens. However, later in the pandemic, gaps emerged between scientific advice emphasising caution, while politicians increasingly became inclined to promote a relaxation of restrictions to serve economic and social values. At this stage, the logics of scientists, who attach value to evidence and prudence, diverge from the logics of politicians, who seek to comfort their voters with good news.”7
Lessons learned
As South Africa has moved out of the acute phase of the pandemic, the lessons learned must be embraced and best practices adopted to inform future pandemic preparedness. The following key lessons were identified:
1. Advisories needed to use the best available evidence rather than wait for the best possible evidence.
Some advisories were revised multiple times, as new evidence emerged. In particular, there was very little local evidence available at the start of the pandemic and new data were being produced daily, often with conflicting results. Advisories were also produced at different times for different reasons. For example, an urgent question regarding the response to an upsurge in cases and whether the alert level needed to be adjusted had to be addressed quickly with the evidence at hand. In some instances, advisories were required within 24 hours or less. However, a more fundamental health systems question, such as on the integration of COVID-19 into routine health systems or the options to address vaccine hesitancy, could benefit from a more extended and extensive review of the available evidence.
2. Transparency was key and should be integral to any future emergency responses.
Advisories were submitted to the Minister for consideration prior to public release. However, in some cases, delays in such release led to confusion as to the scientific basis of executive decisions. The confidentiality of committee debates also needed to be balanced against the need for engagement with the public. This was reflected against a background of extensive public discourse as to the merits and consequences of public health interventions, a discourse that continues to this day. As described above, from March 2022 all advisories were published on a publicly available dedicated website within seven days of receipt by the Minister. The NEML MAC on COVID-19 Therapeutics also set an important precedent with their proactive publication of rapid reviews, which then informed the guidelines developed by the NICD. These technical inputs were not submitted to the Minister of Health or the NDoH prior to being incorporated in guidelines. The chairperson of the NEML MAC on COVID-19 Therapeutics did, however, report to the IMT on their work.
Although the advisories provided by the MAC on COVID-19 were eventually placed in the public domain in a timely manner, there was no explicit public participation step in the development process. Although the TWGs could draw on additional members beyond the MAC itself, these were usually academics or technocrats, not representatives of civil society or the general population. How best to accommodate the public voice in a time-sensitive emergency response remains an open question.
3. Transparency and feedback regarding the use of advisories by government is an important step in the process.
Some of the advisories provided by the MAC on COVID-19 could be directly linked to decisions and actions, such as the revision of topic-specific regulations issued in terms of the Disaster Management Act. Others could not as easily be linked, or were apparently not accepted and actioned. Consistent feedback to the MAC was also important, as their advice was only one of many inputs considered by a complex array of government bodies, across different departments. The quality and timeliness of feedback received from the Minister and NDoH varied considerably over time, and was often deficient or lacking entirely. However, the MAC was also assured by its political principals that its advice was valued. The extent to which purely political considerations contradicted scientific advice is difficult to ascertain, but some issues remained highly contested, perhaps reflecting the range of actors involved. How best to manage cross-border travel was one such issue.
Conclusions and recommendations
The world faces the risk of further pandemics and other public health emergencies and is engaged in high-level negotiations on strengthening global capacity to respond. Three global activities to address pandemic threats are being addressed simultaneously. The first is the proposal for a new Pandemic Accord which is being developed by a WHO-appointed Intergovernmental Negotiating Body tasked with drafting and negotiating a WHO convention, agreement, or other international instrument on pandemic prevention, preparedness and response (https://apps.who.int/gb/inb/). Two other relevant global initiatives that will frame future global pandemic responses include the review and strengthening of the International Health Regulations (2005), and a new agreement on how medical countermeasures should be developed and accessed in future.
This reflection on the role of an advisory structure in the COVID-19 pandemic response has underscored the value of independent and credible scientific advice. The availability of such advice will remain essential. The means to provide independent and credible scientific advice needs to be institutionalised, so that it is ready for the next public health emergency. One option would be to enable a mechanism for rapid mobilisation of an advisory committee through appropriate secondary legislation. As done at global level, a panel of experts could be identified, ready to be called upon rapidly in an emergency, while retaining flexibility to recruit relevant expertise dependent on the context of the crisis.