
Introduction
Population mobility influences the spread of communicable diseases, which challenges public health system capacity in neighbouring countries.1 Advancement of regional, bilateral, and multilateral frameworks and agreements developed by partners at all border system levels can shift policy towards improved alignment of cross-border public health strategies for a coherent response approach.2,3
The US Centers for Disease Control and Prevention (CDC) Global Border Health Team (GBHT) works with countries to strengthen their ability to prevent, detect, and respond to public health events at points of entry (PoEs) and among mobile populations, and to enhance cross-border information-sharing for improved surveillance and strategy alignment.
Jointly implemented by the CDC GBHT and Health Systems Trust (HST), the Border Health Project supported in-country stakeholders from multi-disciplinary departments in eight Southern African Development Community (SADC) Member States (namely Botswana, Eswatini, Lesotho, Mozambique, Namibia, South Africa, Zambia and Zimbabwe) to identify priority areas for border health-system strengthening. These priorities informed the project objectives and activities (as detailed in later sections), and were addressed through capacity-building workshops and regional meetings.
The project approach accounted for the multi-sectoral nature of border health management and the evolution of policies to address public health emergencies by partnering with the World Health Organization (WHO), the East, Central, and Southern Africa Health Community (ECSA-HC), the Africa Centers for Disease Control and Prevention (Africa CDC), and the International Organization for Migration (IOM).
PoEs are strategic spaces for intervention to manage the spread of communicable diseases. They form the nexus of mobility and health where population movement creates joint priority areas for neighbouring countries. While the project’s technical aspects were prompted by the countries’ response to the COVID-19 pandemic, the project concept was aimed at building sustainability into each country’s emergency response and border health monitoring, and epidemiological surveillance of communicable diseases. This was done by describing and mapping mobility patterns and developing procedures for the detection, isolation, management and referral of ill travellers at PoEs.
A range of key international and regional border health strategies and protocols were cited by the participating countries during project implementation. Foremost were the Africa CDC Strategy (2017-2021),4 the WHO International Health Regulations (IHR) of 2005,5 the 1999 SADC Protocol on Health,6 and the One Health approach to addressing zoonotic diseases in countries7,8 jointly formulated by the Food and Agriculture Organization of the United Nations (FAO), the World Organisation for Animal Health (WOAH)[1], and the WHO.
Also listed were guidelines for cross-border collaboration and transportation6,9 and public health capacity-building at ground crossings,10,11 and reports with recommendations on priority communicable diseases such as anthrax,7,12,13 cholera,14–16 COVID-19,6,17,18 HIV,7,19 malaria,6,20,21 plague,22,23 polio,24–26 rabies,7 tuberculosis,6,27 and viral haemorrhagic fevers.7 Reviews on special population groups, i.e. military personnel28 and prisoners,29 were also mentioned.
The chapter presents the findings of semi-structured interviews and an online survey conducted with Border Health Project participants to determine whether and how the project supported improvements in regional collaboration in preparing for and refining responses to limit cross-border disease spread. Also explored were the countries’ perceptions of how their border health systems were strengthened through the project, and whether the trainings were cascaded to stakeholders at their key PoEs.
Methods
The methodologies applied are presented in chronological order to reflect how the project unfolded. Common tools were used throughout the process, from site assessments and audit tools, Geographic Information Systems (GIS), Population Connectivity Across Borders (PopCAB), and these were implemented within an approach that incorporated the WHO and SADC guidelines, the Integrated Disease Surveillance and Response (IDSR) framework, and individual country monitoring tools.
Country need assessments
In-country introductory meetings and PoE site visits were held to assess and collate capacity-building needs; this process informed the development of training plans and workshop content. The assessments were populated by the participating countries, which identified their priorities in driving the capacity-building project agenda.
Regional consultative meetings
Regional meetings held during 2022 supported the eight countries in identifying border health priorities, aligning strategies to strengthen regional cross-border public health information-sharing, and improving co-ordinated public health surveillance, communication, preparedness and response.
The specific objectives of the first regional meeting, held in Zimbabwe from 20 to 24 June 2022, were to:
-
facilitate peer-to-peer sharing of lessons learnt from recent national and regional public health responses (including COVID-19 and polio outbreaks) and identify best practices for responding to public health events with cross-border implications;
-
develop procedures to strengthen cross-border public health information-sharing and co-ordination at national and local levels in support of operationalising existing frameworks; and
-
characterise regional cross-border movement dynamics towards identifying shared priority areas for enhanced cross-border co-ordination.
This meeting enabled participants to share border health best practices, list priority diseases, and articulate existing communication structures and channels for information-sharing. The participants drafted procedures to facilitate the operationalisation of existing cross-border frameworks and bilateral and multilateral agreements. Table 1 lists each participating country’s best practices and challenges.
Mapping exercises helped to illustrate population movement across borders, and the delegates drew up a regional map of bi- and multi-national PoEs per country and overlapping between countries, prioritised for cross-border information-sharing and co-ordination (Figure 1).

Presentations delivered by the CDC GBHT and various partners ‒ Africa CDC, ECSA-HC, the IOM, the SADC, and the WHO ‒ provided perspectives on how existing systems for cross-border collaboration could be strengthened.
Through an iterative and collaborative process, the participants redirected the workshop programme for the second regional meeting (held in South Africa from 12 to 16 September 2022) for closer synergy of the countries’ identified needs. The final agreed objectives resulted in the following outcomes:
-
case definition comparison;
-
refinement of procedures drafted during the first regional meeting;
-
the development of a comprehensive report for participants to share with their respective leadership to advance cross-border co-ordination; and
-
the distribution of a draft Memorandum of Understanding (MoU) template.
Each country presented its input on these core aspects during facilitated group working sessions organised for country- and regional-level deliberation. The group results were synthesised in plenary sessions for documentation purposes.
Training on cross-border health and population mobility
The CDC GBHT developed training materials to capacitate stakeholders with skills and knowledge for responding to public health events at PoEs, and for routinely collecting information on mobile populations.
The project’s skills-development component, delivered from June to August 2022, comprised a PoE capacity-building workshop; training on the PopCAB Toolkit; and orientation on GIS to deepen stakeholders’ understanding of geospatial information on regional cross-border movement dynamics.
Each country sent five delegates from their Ministry of Health and other departments managing border health activities to attend the workshops. They represented departments of Agriculture and Veterinary Services, Immigration, and Health, and in their various capacities play a role in cross-border movement control, disease surveillance including cross-border/Port Health control activities, information-sharing, regulation, and human and animal health sector involvement..
Point-of-entry capacity-building
Two sub-regional workshops for PoEs were conducted, the first in Eswatini from 18 to 23 July 2022, and the second in Lesotho from 26 to 30 July 2022, with 40 participants trained overall.
This training-of-trainers programme focused on building capacity to improve border health systems at PoEs through cascaded training to other Port Health and non-health border staff in the following areas:
-
routine roles and responsibilities;
-
developing and operationalising multi-sectoral public health emergency and response plans (PHERPs) and standard operating procedures (SOPs) in line with the IHR; and
-
implementing exercises to test public health responses at PoEs.
The PoE training consisted of didactic sessions, country presentations, working group exercises to practise applying the guidance gleaned during the training, and plenary sessions. The content covered the IHR, conducting ill-traveller risk assessment, training non-health partners on RING (Recognise, Isolate, Notify, and Give support), developing SOPs and PHERPs at PoEs, and public health exercises to evaluate and strengthen response plans and procedures. The participants also consulted with the facilitators to address areas needing clarity or elaboration. A key resource in this training was a GBHT publication on strengthening comprehensive national and regional border health responses to communicable diseases.30
PopCAB Toolkit and GIS training
The PopCAB training was delivered in two sub-regional workshops, the first in South Africa from 13 to 15 July 2022, and the second in Zimbabwe from 2 to 4 August 2022, for five Ministry of Health representatives from each participating country.
A key GBHT resource used was an approach integrating population mobility patterns and socio-cultural factors in communicable disease preparedness and response.30 The didactic and practical activities included orientation on the PopCAB Toolkit31 ‒ a resource designed to gather and analyse information on population mobility patterns to inform public health interventions – as well as map annotation, data application and processing, and group-work presentations on results from a practice PopCAB.
The PopCAB Toolkit enables identification of routes taken, travellers’ reasons for travel, and the types of travellers moving through an area, to inform response strategies for infectious diseases.
This workshop built the participants’ skills in conducting focus-group discussions and key informant interviews to gather qualitative and geospatial information on country and regional cross-border movement dynamics.
GIS training was held in Gaborone from 15 to 19 August 2022. The country officials were introduced to methods of managing, visualising and analysing qualitative and participatory mapping data on population mobility at local and national levels for sustainability, and were guided on how such data can be used to inform public health interventions.
The intended outcomes of the PoE capacity-building and PopCAB Toolkit trainings were that countries would be equipped to proceed with information-gathering on mobile populations to inform public health interventions and cross-border collaboration; and that countries would establish and/or enhance border health systems with relevant PoE-level SOPs and PHERPs. Where time and budget allowed, the project supported in-country cascade of the trainings to other health and non-health border staff members.
Data collection
This investigation deployed two data-collection methods:
Firstly, responses were extracted from summarised transcriptions of video-recorded, semi-structured interviews conducted with a lead representative from each of the eight countries during the first regional meeting held in Zimbabwe from 20 to 24 June 2022 (Table 2).
The country leads were interviewed by a Division of Global Migration and Quarantine (DGMQ) facilitator. The following question prompts were provided to the interviewees in advance of each 20-minute interview:
-
Name, position and portfolio description
-
The role of their division in monitoring border health and population movement
-
The primary challenges encountered and lessons learnt during the COVID-19 pandemic and/or other disease outbreaks
-
Their insights gleaned during the first regional workshop
-
Their expectations for the forthcoming training.
The team reviewed the video content to identify key themes.
Secondly, a survey with closed and open-ended questions was administered in October/November 2022 to each of the eight countries’ lead representatives (16 in total), using Survey Monkey. The eight questions required a combination of Yes/No and explanatory responses. Respondents were given 14 days to respond. Feedback was solicited on the project’s various trainings and meetings: whether these met the objectives for strengthening capacity at PoEs in the respective countries; how many countries had cascaded trainings to other staff members who had not attended the workshops; and lessons learnt from the trainings and meetings.
Qualitative analysis was done on the 13 responses to the questionnaire. Analysis was conducted in line with a Code Book of identified themes, sub-themes and inclusion criteria, using NVivo software to organise the data for distillation of meaning in relation to the coding strategy. Microsoft Excel was used for quantitative data analysis.
Key findings
Analysis of the video content yielded the following main findings:
-
MoUs finalised between the neighbouring countries are effective mechanisms for cross-border collaboration, and should detail the roles and responsibilities of countries, the conditions under which information will be shared, and the intended use of the information.
-
Border health capacity-building is crucial to ensure improved country preparedness, heightened alertness to situations in neighbouring countries, reduction in the spread of diseases across borders, and optimised disease management in the country of origin.
-
The Border Health Project enabled face-to-face meetings between country counterparts to discuss important issues such as PoE capacities; the project also provided a common framework template for the creation of cross-border MoUs, and operationalised the drafting thereof. This was seen as a vital capacity-building opportunity that highlighted the importance of strengthening cross-border collaboration to manage pandemics. It was noted that the project had been offered at the right juncture following the harrowing experience of countries during the COVID-19 pandemic.
-
The most important aspects of the project support cited were joint identification of challenges and best practices, and collective adoption of these for cross-border collaboration.
“The training was beneficial; it provided support for border health which has always had limited funding in Zimbabwe.”
“We learnt from COVID-19 that each country’s capacity must be strengthened.”
“We don’t know where to start; this meeting provided a common framework and common language.”
“Through this support, we can define communication channels for information- and knowledge-sharing.”
Qualitative analysis of the 13 responses to the survey questionnaire generated the following findings:
PoE capacity-building
The most frequently mentioned topic centred on the PoE capacity-building delivered through the project, with 33 references made regarding completed, current, or planned capacity-building at various PoEs. Capacity-building ranged from border co-ordination and collaboration:
“The trainings integrated border co-ordination, collaboration, [and] role definitions during outbreaks.”
to formalisation of communication structures:
"…training has been conducted for point-of-entry staff to establish structures at that level…"
Some countries expanded on their plans to cascade training and capacity-building to more PoEs:
“Capacity-building is required; the trainings need to be cascaded to the PoE so that all the staff members are on board. The PoE capacity-building training also has to be cascaded to the other PoE staff.”
while others advised that although PoE capacity-building was a priority area, lack of funding prevented cascade of the project training to other PoEs:
“We do not have funding but these are priority areas.”
“Lack of funding…”
“We want to conduct this training, though there is no funding now for the activity.”
Standard operating procedures and Public Health Emergency Response Plans
The second most frequently mentioned theme was the importance of SOPs and PHERPs, with 21 references made. While most countries had SOPs pertaining to the screening of travellers:
“Screening of travellers during outbreaks.”
“SOPs on identification and notification of an ill traveller for PoEs.”
some countries were yet to expand their SOPs for ground crossings:
"Only airports have procedures formulated during COVID-19 but [this] needs to be refined to be holistic plans. Ground crossings do not have [SOPs]."
Some countries had fully developed PHERPs, and these were used as exemplars by other countries during the meetings to gauge their levels of preparedness and to support the development of their own PHERPs:
"The plans were developed during this project and they include cross-border collaboration, co-ordination and data management."
In-country communication
In-country communication channels and structures emerged as a diverse theme across the eight countries. Some respondents indicated that while in-country structures were fully developed, the project had led to the enhancement of certain sections of the structures:
“The Ministry’s communication structures remain the same, but there ha[ve] been deliberate efforts to strengthen the communication with the district level.”
“[The project] enhanced and strengthened the already existing internal reporting and communications structures between district, regional and national levels when responding to a cross-border public health concern.”
Other countries noted that their structures were not fully established and required urgent attention:
“The structures are not fully established but there is an existing high-level structure, but training has been conducted for point-of-entry staff to establish structures at that level.”
Inter-country collaboration
Inter-country collaboration and communication formed a dominant theme that emerged from the feedback. While some countries already had clear structures and agreements in place, the project strengthened them:
"There are clear structures and agreements in place and the regional meetings have strengthened them."
Although there were active cross-border committees in place in certain countries, the responses highlight that data-management and information-sharing across international borders is a crucial component requiring enhancement, as indicated by one of the country respondents:
“Cross-border collaboration committees with countries such as Zimbabwe, Mozambique and Angola [exist], but [are] not distinct on external information-sharing as prior approval is required. MoUs and other collaborative agreements are required to enhance the collaboration…”
For other countries, the project had highlighted the need to update current structures, and to develop MoUs to simplify the process of cross-border collaboration:
“…we are in the process of reviewing our external communication protocols and working with some countries to develop a memorandum of understanding.”
Routine inter-country information-sharing
The need for routine inter-country information-sharing did not feature dominantly in the responses. However, they indicated that the project had provided the countries with a vital platform to discuss important issues pertaining to information-sharing:
"The meetings also helped, as they provided a platform for information-sharing and future cross-border collaboration."
Reference was made to the plans developed during the project to strengthen cross-border co-ordination and information-sharing:
"The plans were developed during this project and they include cross-border collaboration, co-ordination and data management."
Requests for additional border-health capacity-building
The respondents listed their requests for various types of additional capacity-building needed for prioritising any infectious diseases that might present public health threats. Table 3 shows the requests by country.
Quantitative analysis of the survey questionnaire feedback indicated that 13 responses were received from the eight countries. Of these, 10 responses were complete while the remaining three were incomplete. Table 4 sets out the quantified data for the survey responses.
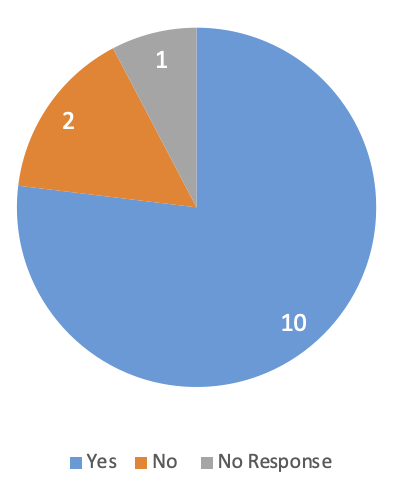
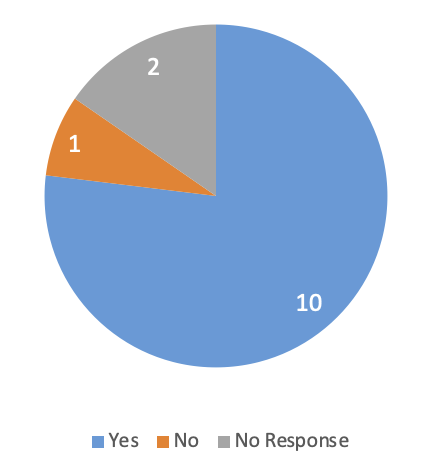
In response to whether countries had managed to establish or enhance clear internal and external communications structures for reporting and responding to a cross-border public health event, 10 respondents (77%) indicated that they had established internal communication structures, two (15%) indicated that they had not, and one respondent (8%) did not answer the question. Ten (77%) indicated that external communication structures had been established, one (8%) indicated that this had not been done, and two (15%) did not answer the question.
Figures 2 and 3 show the percentage of respondents who indicated that internal and external communications structures had been established in their country.


During the sub-regional trainings, country representatives were urged to ensure the roll-out of capacity-building to other colleagues to strengthen border health systems. Of the 13 survey responses, four indicated that their countries had cascaded trainings to other colleagues, while five indicated that they had not, and four did not respond to the question. Mozambique indicated that the IOM and WHO also conducted trainings related to cross-border health issues in their country.
The respondents were asked to list any specific trainings and other PoE activities planned for the near future, and these are presented by country in Table 5. Six of the countries indicated that they had training plans in place, among which were modules for the development of contingency plans and SOPs, risk assessment, and surveillance training. Lesotho and Namibia did not indicate whether they had training plans.
Nine respondents indicated that their countries had PHERPs at PoE level, and four did not answer the question. Nine respondents indicated that their countries had developed SOPs for guidance on emergency public health events, while two participants from Lesotho, one from South Africa, and one from Namibia did not respond to the question.
Conclusions
During the project’s first regional meeting, participants expressed that their countries had become increasingly isolated following the outbreak of COVID-19, and had made unilateral decisions that were often not understood by their neighbouring countries. The survey responses indicate that the project’s face-to-face meetings were therefore critical for enhancing communication at all levels for regional knowledge-building. Moreover, the project provided a valuable platform for facilitating the development of MoUs between neighbouring countries.
Disrupted trade and supply chains caused by border closures to control cross-border disease transmission have been shown to impair livelihoods, and in turn, to impact household health and welfare in African countries.1,32 Understanding the effectiveness of cross-border and PoE health measures used in regional settings can help to inform evidence-based rationales for policy and practice that balance public health goals with other societal needs.
The project’s support for instilling national and regional good practice in internal and inter-country collaboration on disease mitigation, and a renewed focus on data management and information-sharing for public health initiatives, laid a strong foundation for more co-ordinated management of cross-border health measures.
Recommendations
-
The evidence gleaned from the respondents’ feedback indicates that further exploration using key informant interviews could define the countries’ needs for specific interventions and role-players’ transfer of skills developed through the project.
-
All the respondents noted that time constraints had obviated cascade of the PopCAB training at this stage. Three countries expressed interest in doing so, suggesting that this is an area for continued action as a region.
-
Bi-monthly follow-up with country leads to monitor progress with preparedness planning and implementation should be undertaken internally by each country.
-
Master trainers in each country should provide additional PoE capacity-building support where needed.
-
The leads in each country should continue to refine their SOPs and PHERPs.
-
Where they do not exist, MoUs should be established between neighbouring countries. Senior-level implementers who took part in the training undertook to engage with relevant ministry principals to finalise such MoUs.
-
Timeframes for inter-country communication (e.g. monthly or bi-annual meetings) should be established by the respective countries.
DGMQ and the HST should engage with countries for post-project analysis to measure the sustainability of the project, subject to availability of funding. A regional body should bring countries together to chart a way forward for standardising use of tools and frameworks for policy coherence. Dialogue among member states for such harmonisation should be facilitated through a regional bloc such as SADC.
External partners such as the IOM, SADC, ECSA-HC, and WHO should facilitate clearly delineated guidance.
Acknowledgements
The authors are grateful to their CDC colleagues, Dr Rebecca Merrill, Ms Sarah Ward, Dr Kiswendsida Sawadogo, and Ms Chloe Crocker, and to their HST colleague, Ms Noluthando Ndlovu, for their support and contribution to the project and this chapter. The authors also acknowledge the United States Centers for Disease Control and Prevention for funding the project, and all representatives of the participating countries and regional bodies for their invaluable insights and committed effort.
Founded as Office International des Epizooties (OIE)