Introduction
The South African Health Review 2022 focuses on the response, mitigation, recovery, and health-systems-strengthening strategies employed to rebuild the health system in South Africa in the wake of the COVID-19 pandemic. Information systems form a key health-systems building block. The World Health Organization (WHO) has described a well-functioning health-information system as “one that ensures the production, analysis, dissemination and use of reliable and timely information on health determinants, health system performance and health status”.1 This chapter examines the available health-information data sources in South Africa, with a particular focus on whether they have strengthened during and after the acute phase of the COVID-19 pandemic.
An upcoming book written by Dr Jonathan Kennedy, entitled Pathogenesis: How Germs Made History, examines the role of eight pathogens in shaping global history. Kennedy has been quoted as saying: “We’re living in a golden age for microbes. Population densities are increasing, people are moving more quickly around the world, the climate is changing. We’ve seen the emergence not just of COVID-19, but of HIV/AIDS, Zika, Dengue fever, SARS and Ebola. It seems now that we won’t be able to conquer infectious diseases. Rather, we’re going to have to learn to deal with the new diseases that periodically arrive to threaten us.”2 There are indications that the world is starting to ‘live with’ SARS-CoV-2, the novel coronavirus responsible for COVID-19. However, whether global and national health systems will be left more resilient, better resourced and more agile, or whether they will regress to the state of fragmentation and vulnerability exposed in 2020, remains to be seen.
The immediate signals are less than convincing. Health-information systems created under pandemic pressures are being allowed to close, are being defunded, or are simply becoming less timely and less effective. The lessons of this pandemic are at risk of being lost, even before the pandemic has formally been declared over. In a 2022 commentary, Pillay et al. pointed out that the post-COVID-19 recovery effort not only aims to ensure that services recover to “2019 levels at least”, but “to use the lessons from the COVID-19 response to radically transform the SA health system”.3
Data Sources
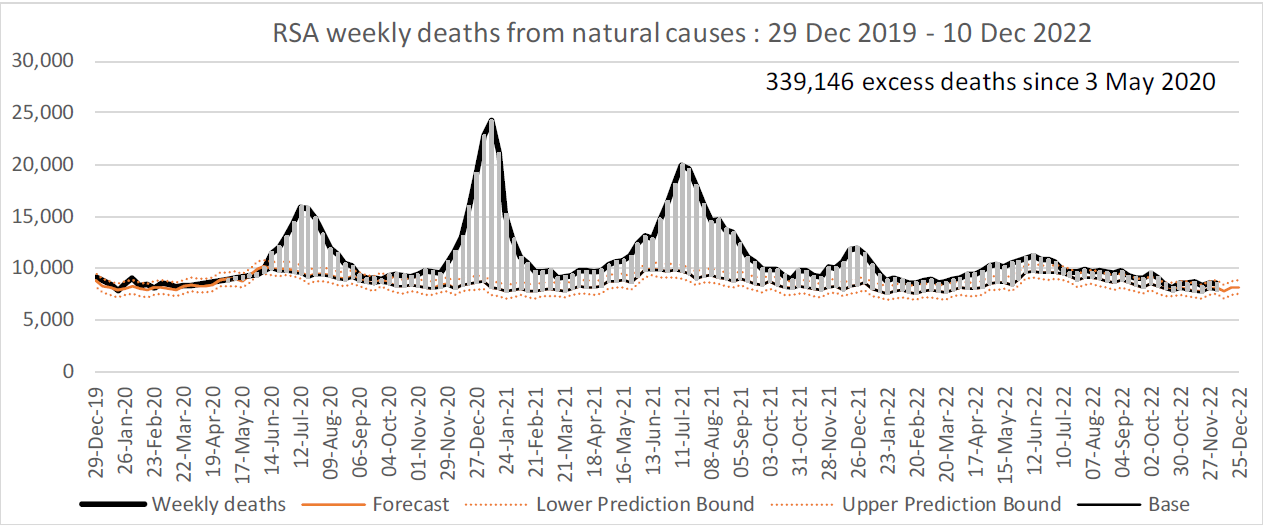
Box 1 shows the key new or updated sources relied on at both international and national level. Specific references and the current indicator definitions are provided in the data tables in the chapter. Many of the indicators have been normalised using population denominators. Routine data were obtained from web-based District Health Information System (WebDHIS), covering especially the 2021/22 financial year, which ran from April 2021 to March 2022. In a number of the sections below, the difference between expected and actual routine measures has been depicted graphically. The expected trends have been forecast using the Holt-Winters method.4,5
As highlighted in previous editions of the Review, caution is warranted when using data that are presented for several years. As data may be drawn from multiple sources, care should be taken in assessing trends and changes over time. Differences in methodology and data presentation may make comparisons challenging. Data from regular surveys may also not be comparable over time. In some cases, revised data for a historical time series may be released, for example with the Statistics South Africa General Household Surveys. This may result in different values being published than in previous editions of the Review. When using time-series data, the most recent revisions should be obtained from the online database and not from previous printed editions of this chapter.
Box 1.Key new or updated health data sources, 2022
| International |
South African |
- World Health Statistics 2022
- Human Development Report 2021/2022
- World Malaria Report 2022
- Global Fund Results Report 2021
- Global Tuberculosis Report 2022
- The State of the World’s Children 2021
- Mental State of the World Report 2021
- The State of Air Quality and Health Impacts in Africa 2022
- Joint United Nations Programme on HIV and AIDS (UNAIDS) Update 2022
- Global COVID-19 data repositories and dashboards
- Global Cancer Incidence, Mortality and Prevalence (GLOBOCAN) 2020
- International Diabetes Federation (IDF) Diabetes Atlas 2021
|
- Web-based District Health Information System (webDHIS)
- Tier.Net, now incorporating the Electronic TB Register
- Electronic Drug-Resistant TB Register (EDRWeb)
- Stats SA Mid-year population estimates 2022
- Stats SA General Household Survey (GHS) 2021
- Stats SA Labour Force Surveys up to the 4th quarter of 2022
- Recorded live births 2020 & 2021
- National Treasury health expenditure data
- Personnel Administration System (PERSAL)
- Thembisa v4.5 HIV and AIDS model
- South African Community Epidemiology Network on Drug Use (SACENDU)
- Council for Medical Schemes Annual Report 2021/22
- Blue Drop Progress Report 2022
- Rapid Mortality and Surveillance Report 2019 & 2020
- Surveillance data, surveillance bulletins and other reports issued by the National Institute for Communicable Diseases (NICD)
|
1. Demographic indicators
There has been a lot of speculation about the impact that the COVID-19 pandemic will have on demographic trends, particularly because population ageing is driven by fertility and mortality trends. In European and other Western countries, data suggest that births had fallen sharply by the end of 2020.6 This finding is consistent with responses to pandemics in the past, where a sharp decline in births has typically been followed by gradual increases in births and then a ‘baby boom’. However, previous pandemics have also been characterised by high mortality among younger people and those of childbearing age. COVID-related deaths have been more prevalent in the older population, therefore the motivation for high birth rates to replace those who have died is not there. More than anything, the disruption of maternal health services, particularly a lack of contraception in low- and middle-income countries (LMICs) due to lockdowns, and interruptions to health services and supplies, could have inadvertently led to as many as 1.4 million unintended pregnancies.7
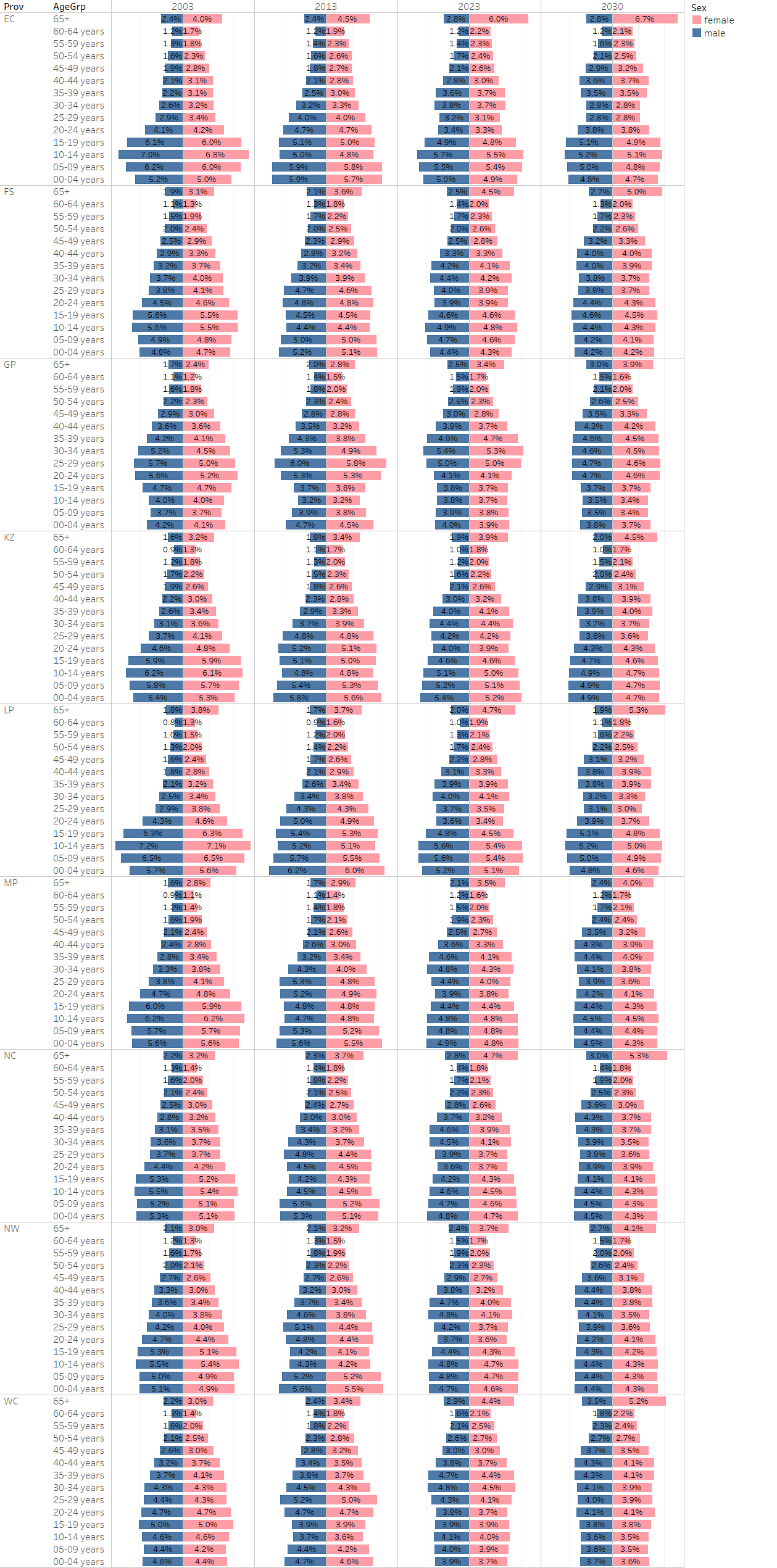
South Africa has the highest proportion of elderly people among countries in the African region.8 Although population ageing is still in its early stages in the country, the proportion of persons aged 60 years and older is increasing over time, as shown in the South African national population pyramid (Figure 1). This will ultimately have implications for the health system overall as it will intensify the disease burden related to multiple chronic conditions.9 Consequently, programmes and policies to address this ageing population should be prioritised as older adults have different health needs to a younger population. In addition, the country’s quadruple burden of communicable and non-communicable diseases also manifests in high levels of unhealthy ageing.9

Figure 1.Population pyramid by province, 2003-2030
Source: webDHIS-NDoH 2000-2030 population time series10 (received August 2020).
The total population in South Africa is estimated to have increased from 60.1 million in 2021 to 60.6 million people in 2022, with females still accounting for 51.1% of the population (Table 1). South Africa’s expected national Census could not be completed in 2021 because of the COVID-19 pandemic. The Census was postponed to 2022, and has been completed. However, the 2022 mid-year estimates do not take account of the Census data, as these figures will only be released later in 2023. The estimates are therefore continuations of the projections from the 2011 Census. As estimated, the province with the highest share of the country’s population remains Gauteng (26.6%, 16.1 million people), while the smallest share of the population is still found in the Northern Cape (2.2%, 1.31 million people). The population density has also increased in Gauteng, from 870 to 886 people per square kilometre.11 The 2022 Census may well present data showing even more marked internal migration, with populations in more rural provinces, depleted by migration, moving to the economic hubs of Gauteng and the Western Cape. Such changes in population will have major implications for the allocation of funds from the fiscus, in the form of the equitable share formula.
Table 1.Demographic indicators by province, 2020-2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Ageing index |
2021 |
both sexes mid-year |
21,6 |
25,1 |
23,2 |
23,0 |
17,7 |
18,6 |
18,6 |
23,8 |
20,6 |
28,2 |
a |
| 2022 |
both sexes mid-year |
22,1 |
25,3 |
23,5 |
23,5 |
17,6 |
18,8 |
19,7 |
24,1 |
20,8 |
29,4 |
b |
| Annual population growth rate |
2021 |
both sexes mid-year |
1,0 |
|
|
|
|
|
|
|
|
|
a |
| 2022 |
both sexes mid-year |
1,1 |
|
|
|
|
|
|
|
|
|
b |
| Crude death rate (deaths per 1 000 population) |
2020 |
both sexes all ages mid-year |
8,7 |
|
|
|
|
|
|
|
|
|
c |
| 2021 |
both sexes mid-year |
11,5 |
|
|
|
|
|
|
|
|
|
a |
| 2022 |
both sexes all ages mid-year |
11,0 |
|
|
|
|
|
|
|
|
|
b |
| Live birth occurrences registered |
2020 |
vital registration total |
1 003 307 |
114 881 |
46 265 |
228 299 |
205 781 |
132 893 |
95 898 |
23 540 |
57 979 |
97 771 |
d |
| 2021 |
vital registration total |
1 087 526 |
129 381 |
52 260 |
247 378 |
223 712 |
137 780 |
104 061 |
27 980 |
61 605 |
103 368 |
e |
| Population |
2021 |
both sexes all ages mid-year |
60 142 979 |
6 676 590 |
2 932 441 |
15 810 388 |
11 513 575 |
5 926 724 |
4 743 584 |
1 303 047 |
4 122 854 |
7 113 776 |
a |
| both sexes all ages Stats SA 2019-30 FinYr total |
60 354 419 |
6 544 060 |
3 004 609 |
15 874 780 |
11 738 948 |
5 959 813 |
4 745 703 |
4 176 475 |
1 269 273 |
7 040 757 |
f |
| female all ages mid-year |
30 754 931 |
|
|
|
|
|
|
|
|
|
a |
| male all ages mid-year |
29 388 047 |
|
|
|
|
|
|
|
|
|
a |
| 2022 |
both sexes all ages Stats SA 2019-30 FinYr total |
61 220 537 |
6 551 888 |
3 020 662 |
16 271 412 |
11 847 316 |
6 004 534 |
4 815 440 |
4 242 620 |
1 283 976 |
7 182 690 |
f |
| both sexes mid-year |
60 604 992 |
6 676 691 |
2 921 611 |
16 098 571 |
11 538 325 |
5 941 439 |
4 720 497 |
1 308 734 |
4 186 984 |
7 212 142 |
b |
| female mid-year |
30 980 110 |
|
|
|
|
|
|
|
|
|
b |
| male mid-year |
29 624 882 |
|
|
|
|
|
|
|
|
|
b |
| Population % by province |
2021 |
both sexes all ages mid-year |
100,0 |
11,1 |
4,9 |
26,3 |
19,1 |
9,9 |
7,9 |
2,2 |
6,9 |
11,8 |
a |
| 2022 |
both sexes mid-year |
100,0 |
11,0 |
4,8 |
26,6 |
19,0 |
9,8 |
7,8 |
2,2 |
6,9 |
11,9 |
b |
| Population density |
2021 |
mid-year |
49,3 |
39,5 |
22,6 |
869,8 |
122,0 |
47,1 |
62,0 |
3,5 |
39,3 |
54,9 |
a |
| 2022 |
mid-year |
49,6 |
39,5 |
22,5 |
885,6 |
122,3 |
47,2 |
61,7 |
3,5 |
39,9 |
55,7 |
b |
| Population under 1 year |
2021/22 |
both sexes under 1 year DHIS |
1 139 382 |
130 901 |
50 371 |
263 761 |
255 744 |
124 972 |
96 828 |
25 739 |
81 115 |
109 951 |
g |
Public sector dependent
(uninsured) population |
2020 |
both sexes all ages GHS |
49 798 387 |
5 955 518 |
2 501 372 |
11 873 601 |
10 005 297 |
5 339 978 |
4 145 892 |
1 051 559 |
3 450 829 |
5 399 356 |
h |
| both sexes all ages non med schemes |
51 256 046 |
6 012 497 |
2 535 990 |
12 375 348 |
10 223 911 |
5 454 669 |
4 192 033 |
1 121 438 |
3 666 797 |
5 727 477 |
i |
| 2021 |
both sexes all ages GHS |
50 847 588 |
5 968 962 |
2 445 388 |
12 234 914 |
10 326 801 |
5 454 241 |
4 290 932 |
1 052 222 |
3 546 375 |
5 502 864 |
j |
| non med scheme |
51 599 090 |
6 209 323 |
2 804 747 |
9 820 128 |
9 922 960 |
5 644 367 |
4 437 267 |
1 282 559 |
3 977 635 |
6 130 321 |
k |
| Total fertility rate |
2022 |
both sexes mid-year |
2,3 |
2,9 |
2,3 |
1,8 |
2,5 |
3,0 |
2,3 |
2,6 |
2,5 |
2,0 |
b |
Reference notes
a Stats SA MYE 2021.12
b Stats SA MYE 2022.11
c Stats SA MYE 2020.13
d Recorded Live Births 2020.14
e Recorded Live Births 2021.15
f Pop Est 2019-30.
g webDHIS.10
h Stats SA GHS 2019.16
i Medical Schemes 2020-21.17
j GHS 2021.18
k Medical Schemes 2021-22.19
Definitions
- Population [Number]: Total number of people. Projected population figures are based on various projection models attempting to quantify the expected effects of HIV and AIDS on population growth.
- Adolescent fertility rate (per 1 000 girls aged 15-19 years) [per 1 000 girls aged 15-19 years]: Annual number of births to women aged 15-19 years per 1 000 women in that age group. Also referred to as the age-specific fertility rate for women aged 15-19 years.
- Ageing index [Number]: Ratio of the number of people 65+ to the number under 15 years, i.e. a value of 16 means there are 16 people aged 65 and over for every 100 under 15 years of age. Calculated as ([65+/0-14]*100).
- Annual population growth rate [Percentage]: The rate at which the population is increasing or decreasing in a given year expressed as a percentage of the base population size. It takes into consideration all the components of population growth, namely births, deaths and migration.
- Crude death rate (deaths per 1 000 population) [per 1 000 population]: Number of deaths in a year per 1 000 population.
- Live birth occurrences registered [Number]: The number of live birth occurrences registered.
- Population % by province [Percentage]: Proportion of South African population in each province (calculated from population per province and population for whole of South Africa).
- Population density [people per km2]: The number of people per square kilometre.
- Population under 1 year [Number]: Population under 1 year of age.
- Public sector dependent (uninsured) population [Number]: This is an adjustment of the total population to the number assumed to be dependent on services in the public health sector based on medical scheme (health insurance) coverage. It is calculated by subtracting the number of people with medical scheme cover (determined from medical scheme membership reports, or surveys indicating percentage of population on medical schemes) from the total population.
- Total fertility rate [Number]: The average number of children that a woman gives birth to in her lifetime, assuming that the prevailing rates remain unchanged.
COVID-19 mortality rates dramatically increased the crude death rate in South Africa within just a year from 8.7 deaths per 1000 population in 2000 to 11.5 per 1000 population in 2021. However, in 2022 the modelled crude death rate decreased slightly to 11.0, which could be signalling a recovery post-COVID.11
The Council for Medical Schemes (CMS)20 and the most recent General Household Survey18 reported on the number of medical scheme beneficiaries in 2021. According to the CMS, the number of beneficiaries covered by medical schemes increased by 0.5% between 2020 and 2021; however, overall, both estimates indicated a greater increase in the number of public sector-dependent (uninsured) population.
Table 2 and Table 3 show the webDHIS 2021/22 population estimates per 5-year age band per province, and the population estimates under 1 year of age by district, respectively. Table 4 shows the total and uninsured national, provincial and district population estimates.
Table 2.National and provincial population estimates by age group, 2022
|
Data Age group
|
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
ZA |
| 00-04 years |
672 324 |
255 736 |
1 312 439 |
1 254 648 |
640 842 |
474 862 |
126 615 |
401 940 |
559 465 |
5 698 871 |
| 05-09 years |
742 073 |
275 225 |
1 269 176 |
1 206 334 |
683 923 |
464 812 |
122 417 |
403 240 |
580 581 |
5 747 781 |
| 10-14 years |
754 831 |
286 436 |
1 232 104 |
1 184 767 |
672 127 |
468 020 |
120 660 |
407 962 |
587 345 |
5 714 252 |
| 15-19 years |
641 423 |
261 710 |
1 172 725 |
1 054 280 |
560 776 |
417 641 |
111 696 |
359 788 |
547 677 |
5 127 716 |
| 20-24 years |
446 362 |
226 710 |
1 361 696 |
942 756 |
438 857 |
379 056 |
95 907 |
308 020 |
544 816 |
4 744 180 |
| 25-29 years |
448 862 |
234 559 |
1 676 705 |
1 007 870 |
459 359 |
415 475 |
102 623 |
340 336 |
627 099 |
5 312 888 |
| 30-34 years |
509 302 |
255 819 |
1 765 548 |
1 037 819 |
503 828 |
449 514 |
115 352 |
383 469 |
684 309 |
5 704 960 |
| 35-39 years |
477 079 |
237 118 |
1 551 317 |
922 228 |
467 497 |
415 064 |
109 589 |
359 327 |
651 745 |
5 190 964 |
| 40-44 years |
376 074 |
185 817 |
1 204 748 |
691 506 |
373 113 |
318 885 |
86 589 |
288 422 |
524 513 |
4 049 667 |
| 45-49 years |
316 706 |
154 270 |
958 401 |
556 498 |
302 871 |
250 403 |
70 290 |
234 740 |
437 730 |
3 281 909 |
| 50-54 years |
272 493 |
133 078 |
766 418 |
444 613 |
242 391 |
199 836 |
59 743 |
192 645 |
384 670 |
2 695 887 |
| 55-59 years |
247 062 |
115 550 |
631 025 |
384 910 |
207 573 |
166 681 |
50 210 |
162 607 |
329 427 |
2 295 045 |
| 60-64 years |
228 979 |
96 863 |
518 950 |
322 761 |
170 566 |
129 856 |
42 317 |
134 595 |
268 461 |
1 913 348 |
| 65-69 years |
189 870 |
78 534 |
395 579 |
254 007 |
139 852 |
101 388 |
34 838 |
100 365 |
201 474 |
1 495 907 |
| 70-74 years |
140 214 |
57 013 |
274 282 |
192 803 |
104 293 |
71 045 |
25 762 |
67 595 |
144 581 |
1 077 588 |
| 75-79 years |
98 996 |
35 341 |
164 093 |
123 743 |
65 202 |
41 869 |
17 194 |
44 547 |
94 417 |
685 402 |
| 80+ years |
148 765 |
30 699 |
106 946 |
101 622 |
91 372 |
50 653 |
19 006 |
41 681 |
75 211 |
665 955 |
| Total |
6 711 415 |
2 920 478 |
16 362 152 |
11 683 165 |
6 124 442 |
4 815 060 |
1 310 808 |
4 231 279 |
7 243 521 |
61 402 320 |
Source: webDHIS Pop Est 2000-30.
Table 3.Population estimates under 1 year of age by district, 2022/23
| Province |
District |
Female under
1 year
|
Male under
1 year
|
Population
under 1
|
| EC |
BUF: Buffalo City MM |
5 382 |
5 523 |
10 905 |
| |
DC10: Sarah Baartman DM |
3 587 |
3 622 |
7 209 |
| |
DC12 : Amathole DM |
7 308 |
7 535 |
14 843 |
| |
DC13: C Hani DM |
6 628 |
6 815 |
13 443 |
| |
DC14: Joe Gqabi DM |
3 081 |
3 133 |
6 214 |
| |
DC15: OR Tambo DM |
19 849 |
20 403 |
40 252 |
| |
DC44: A Nzo DM |
10 992 |
11 181 |
22 173 |
| |
NMA : N Mandela Bay MM |
8 078 |
8 095 |
16 173 |
| FS |
DC16: Xhariep DM |
1 268 |
1 287 |
2 555 |
| |
DC18: Lejweleputswa DM |
5 325 |
5 328 |
10 653 |
| |
DC19: T Mofutsanyana DM |
7 232 |
7 336 |
14 568 |
| |
DC20: Fezile Dabi DM |
4 021 |
4 078 |
8 099 |
| |
MAN : Mangaung MM |
7 092 |
7 389 |
14 481 |
| GP |
DC42: Sedibeng DM |
7 298 |
7 556 |
14 854 |
| |
DC48: West Rand DM |
7 410 |
7 706 |
15 116 |
| |
EKU : City of Ekurhuleni MM |
34 209 |
34 970 |
69 179 |
| |
JHB : Johannesburg MM |
48 794 |
49 799 |
98 593 |
| |
TSH : Tshwane MM |
31 681 |
32 573 |
64 254 |
| KZ |
DC21: Ugu DM |
9 322 |
9 446 |
18 768 |
| |
DC22: uMgungundlovu DM |
11 349 |
11 575 |
22 924 |
| |
DC23: uThukela DM |
8 324 |
8 626 |
16 950 |
| |
DC24: uMzinyathi DM |
7 835 |
8 165 |
16 000 |
| |
DC25: Amajuba DM |
6 343 |
6 555 |
12 898 |
| |
DC26: Zululand DM |
11 007 |
11 400 |
22 407 |
| |
DC27: uMkhanyakude DM |
8 805 |
8 941 |
17 746 |
| |
DC28: King Cetshwayo DM |
11 216 |
11 552 |
22 768 |
| |
DC29: iLembe DM |
7 699 |
7 856 |
15 555 |
| |
DC43: Harry Gwala DM |
6 243 |
6 374 |
12 617 |
| |
ETH : eThekwini MM |
37 009 |
38 396 |
75 405 |
| LP |
DC33: Mopani DM |
12 416 |
12 951 |
25 367 |
| |
DC34: Vhembe DM |
14 902 |
15 513 |
30 415 |
| |
DC35: Capricorn DM |
13 361 |
13 909 |
27 270 |
| |
DC36: Waterberg DM |
6 623 |
6 863 |
13 486 |
| |
DC47: Sekhukhune DM |
14 107 |
14 653 |
28 760 |
| MP |
DC30: G Sibande DM |
12 643 |
12 883 |
25 526 |
| |
DC31: Nkangala DM |
14 498 |
14 931 |
29 429 |
| |
DC32: Ehlanzeni DM |
19 827 |
20 302 |
40 129 |
| NC |
DC6 : Namakwa DM |
928 |
916 |
1 844 |
| |
DC7 : Pixley Ka Seme DM |
2 090 |
2 141 |
4 231 |
| |
DC8 : ZF Mgcawu DM |
2 548 |
2 524 |
5 072 |
| |
DC9 : Frances Baard DM |
3 963 |
4 083 |
8 046 |
| |
DC45: JT Gaetsewe DM |
3 025 |
3 062 |
6 087 |
| NW |
DC37: Bojanala Platinum DM |
17 818 |
18 060 |
35 878 |
| |
DC38: NM Molema DM |
8 620 |
8 682 |
17 302 |
| |
DC39: RS Mompati DM |
5 929 |
6 105 |
12 034 |
| |
DC40: Dr K Kaunda DM |
7 683 |
7 754 |
15 437 |
| WC |
CPT : Cape Town MM |
34 900 |
36 470 |
71 370 |
| |
DC1 : West Coast DM |
3 847 |
3 929 |
7 776 |
| |
DC2 : Cape Winelands DM |
7 848 |
8 167 |
16 015 |
| |
DC3 : Overberg DM |
2 583 |
2 749 |
5 332 |
| |
DC4 : Garden Route DM |
4 989 |
5 202 |
10 191 |
| |
DC5 : Central Karoo DM |
578 |
594 |
1 172 |
| Total |
|
560 113 |
575 658 |
1 135 771 |
Table 4.Population estimates: modelled estimates for medical schemes coverage and uninsured population national, provincial and district, 2019-2023
|
Total Population (DHIS Pop Est 2000-30) |
Med schemes coverage (Insight Actuaries model 2019) |
Uninsured Calculated |
| 2019 |
2020 |
2021 |
2022 |
2023 |
2018 |
2019 |
2020 |
2021 |
2022 |
2023 |
| Country |
ZA |
58 979 654 |
59 797 656 |
60 604 086 |
61 402 320 |
62 197 960 |
15,4 |
49 896 787 |
50 588 817 |
51 271 057 |
51 946 363 |
52 619 474 |
| Province |
EC |
6 711 899 |
6 713 318 |
6 714 789 |
6 711 415 |
6 709 060 |
9,8 |
6 054 133 |
6 055 413 |
6 056 740 |
6 053 696 |
6 051 572 |
| FS |
2 890 007 |
2 900 278 |
2 910 130 |
2 920 478 |
2 930 982 |
13,5 |
2 499 856 |
2 508 740 |
2 517 262 |
2 526 213 |
2 535 299 |
| GP |
15 268 630 |
15 635 579 |
15 997 809 |
16 362 152 |
16 723 636 |
24,6 |
11 512 547 |
11 789 227 |
12 062 348 |
12 337 063 |
12 609 622 |
| KZ |
11 319 610 |
11 441 785 |
11 563 182 |
11 683 165 |
11 801 471 |
11,2 |
10 051 814 |
10 160 305 |
10 268 106 |
10 374 651 |
10 479 706 |
| LP |
5 993 527 |
6 039 032 |
6 084 467 |
6 124 442 |
6 165 877 |
7,2 |
5 561 993 |
5 604 222 |
5 646 385 |
5 683 482 |
5 721 934 |
| MP |
4 609 880 |
4 680 103 |
4 748 543 |
4 815 060 |
4 880 047 |
12,5 |
4 033 645 |
4 095 090 |
4 154 975 |
4 213 178 |
4 270 041 |
| NC |
1 267 621 |
1 282 813 |
1 297 034 |
1 310 808 |
1 324 275 |
15,1 |
1 076 210 |
1 089 108 |
1 101 182 |
1 112 876 |
1 124 309 |
| NW |
4 043 350 |
4 107 283 |
4 169 094 |
4 231 279 |
4 293 016 |
11,9 |
3 562 191 |
3 618 516 |
3 672 972 |
3 727 757 |
3 782 147 |
| WC |
6 875 130 |
6 997 465 |
7 119 038 |
7 243 521 |
7 369 596 |
20,1 |
5 493 229 |
5 590 975 |
5 688 111 |
5 787 573 |
5 888 307 |
| District |
BUF |
799 711 |
798 388 |
796 759 |
794 314 |
791 614 |
22,4 |
620 576 |
619 549 |
618 285 |
616 388 |
614 292 |
| CPT |
4 510 747 |
4 598 783 |
4 686 530 |
4 776 492 |
4 867 548 |
22,2 |
3 509 361 |
3 577 853 |
3 646 120 |
3 716 111 |
3 786 952 |
| DC1 |
455 676 |
463 390 |
471 043 |
478 958 |
487 115 |
17,3 |
376 844 |
383 224 |
389 553 |
396 098 |
402 844 |
| DC2 |
925 999 |
942 232 |
958 398 |
974 747 |
991 117 |
16,4 |
774 135 |
787 706 |
801 221 |
814 888 |
828 574 |
| DC3 |
294 278 |
299 764 |
305 203 |
310 662 |
316 173 |
16,4 |
246 016 |
250 603 |
§§ |
259 713 |
264 321 |
| DC4 |
614 134 |
618 954 |
623 516 |
628 217 |
633 013 |
16,5 |
512 802 |
516 827 |
520 636 |
524 561 |
528 566 |
| DC5 |
74 296 |
74 342 |
74 348 |
74 445 |
74 630 |
12,5 |
65 009 |
65 049 |
65 055 |
65 139 |
65 301 |
| DC6 |
113 937 |
114 035 |
114 077 |
114 245 |
114 367 |
17,5 |
93 998 |
94 079 |
94 114 |
94 252 |
94 353 |
| DC7 |
204 290 |
206 326 |
208 167 |
209 912 |
211 609 |
13,1 |
177 528 |
179 297 |
180 897 |
182 414 |
183 888 |
| DC8 |
273 681 |
278 104 |
282 362 |
286 400 |
290 296 |
15,8 |
230 439 |
234 164 |
237 749 |
241 149 |
244 429 |
| DC9 |
410 232 |
414 190 |
417 771 |
421 181 |
424 540 |
15,7 |
345 826 |
349 162 |
352 181 |
355 056 |
357 887 |
| DC10 |
478 448 |
480 810 |
483 024 |
484 665 |
486 523 |
8,8 |
436 345 |
438 499 |
440 518 |
442 014 |
443 709 |
| DC12 |
804 398 |
795 781 |
787 417 |
778 884 |
770 438 |
4,3 |
769 809 |
761 562 |
753 558 |
745 392 |
737 309 |
| DC13 |
741 095 |
731 081 |
721 434 |
712 004 |
702 218 |
4,9 |
704 781 |
695 258 |
686 084 |
677 116 |
667 809 |
| DC14 |
344 401 |
342 580 |
340 685 |
338 445 |
336 219 |
5,0 |
327 181 |
325 451 |
323 651 |
321 523 |
319 408 |
| DC15 |
1 508 997 |
1 524 972 |
1 541 080 |
1 555 812 |
1 571 532 |
4,2 |
1 445 619 |
1 460 923 |
1 476 355 |
1 490 468 |
1 505 528 |
| DC16 |
126 989 |
127 071 |
127 119 |
127 251 |
127 471 |
10,5 |
113 655 |
113 729 |
113 772 |
113 890 |
114 087 |
| DC18 |
642 629 |
643 043 |
643 503 |
644 397 |
645 123 |
12,0 |
565 514 |
565 878 |
566 283 |
567 069 |
567 708 |
| DC19 |
755 188 |
755 842 |
756 396 |
757 178 |
758 118 |
9,2 |
685 711 |
686 305 |
686 808 |
687 518 |
688 371 |
| DC20 |
504 155 |
505 057 |
505 879 |
506 744 |
507 595 |
13,2 |
437 607 |
438 389 |
439 103 |
439 854 |
440 592 |
| DC21 |
804 993 |
816 195 |
827 384 |
838 645 |
850 311 |
7,1 |
747 838 |
758 245 |
768 640 |
779 101 |
789 939 |
| DC22 |
1 123 554 |
1 137 023 |
1 150 285 |
1 163 352 |
1 177 092 |
11,0 |
999 963 |
1 011 950 |
1 023 754 |
1 035 383 |
1 047 612 |
| DC23 |
704 433 |
706 771 |
708 994 |
711 516 |
714 070 |
6,4 |
659 349 |
661 538 |
663 618 |
665 979 |
668 370 |
| DC24 |
557 752 |
563 568 |
569 454 |
575 760 |
582 409 |
5,4 |
527 633 |
533 135 |
538 703 |
544 669 |
550 959 |
| DC25 |
558 701 |
565 495 |
572 008 |
577 873 |
583 415 |
7,4 |
517 357 |
523 648 |
529 679 |
535 110 |
540 242 |
| DC26 |
858 938 |
863 111 |
867 237 |
872 128 |
877 196 |
5,2 |
814 273 |
818 229 |
822 141 |
826 777 |
831 582 |
| DC27 |
671 378 |
676 068 |
680 655 |
685 592 |
690 192 |
5,0 |
637 809 |
642 265 |
646 622 |
651 312 |
655 682 |
| DC28 |
960 065 |
964 828 |
969 742 |
975 004 |
980 188 |
8,7 |
876 539 |
880 888 |
885 374 |
890 179 |
894 912 |
| DC29 |
671 846 |
680 361 |
688 960 |
696 590 |
703 372 |
8,6 |
614 067 |
621 850 |
629 709 |
636 683 |
642 882 |
| DC30 |
1 218 483 |
1 240 644 |
1 262 612 |
1 283 719 |
1 304 284 |
13,1 |
1 058 862 |
1 078 120 |
1 097 210 |
1 115 552 |
1 133 423 |
| DC31 |
1 580 378 |
1 613 205 |
1 645 648 |
1 677 409 |
1 708 843 |
14,8 |
1 346 482 |
1 374 451 |
1 402 092 |
1 429 152 |
1 455 934 |
| DC32 |
1 811 019 |
1 826 254 |
1 840 283 |
1 853 932 |
1 866 920 |
10,2 |
1 626 295 |
1 639 976 |
1 652 574 |
1 664 831 |
1 676 494 |
| DC33 |
1 209 120 |
1 218 016 |
1 226 939 |
1 234 474 |
1 241 931 |
6,8 |
1 126 900 |
1 135 191 |
1 143 507 |
1 150 530 |
1 157 480 |
| DC34 |
1 460 085 |
1 474 045 |
1 488 161 |
1 501 251 |
1 514 770 |
6,6 |
1 363 719 |
1 376 758 |
1 389 942 |
1 402 168 |
1 414 795 |
| DC35 |
1 344 562 |
1 349 214 |
1 353 845 |
1 357 666 |
1 361 654 |
8,3 |
1 232 963 |
1 237 229 |
1 241 476 |
1 244 980 |
1 248 637 |
| DC36 |
763 309 |
769 853 |
776 172 |
781 264 |
786 231 |
9,1 |
693 848 |
699 796 |
705 540 |
710 169 |
714 684 |
| DC37 |
1 884 307 |
1 929 057 |
1 972 917 |
2 015 765 |
2 058 230 |
14,0 |
1 620 504 |
1 658 989 |
1 696 709 |
1 733 558 |
1 770 078 |
| DC38 |
901 629 |
906 601 |
910 841 |
916 394 |
922 575 |
9,7 |
814 171 |
818 661 |
822 489 |
827 504 |
833 085 |
| DC39 |
470 086 |
471 910 |
473 588 |
475 637 |
477 280 |
7,3 |
435 770 |
437 461 |
439 016 |
440 915 |
442 439 |
| DC40 |
787 328 |
799 715 |
811 748 |
823 483 |
834 931 |
12,8 |
686 550 |
697 351 |
707 844 |
718 077 |
728 060 |
| DC42 |
960 427 |
963 811 |
966 230 |
968 999 |
972 188 |
20,8 |
760 658 |
763 338 |
765 254 |
767 447 |
769 973 |
| DC43 |
503 616 |
506 908 |
510 113 |
513 778 |
517 618 |
5,6 |
475 414 |
478 521 |
481 547 |
485 006 |
488 631 |
| DC44 |
826 587 |
828 210 |
830 067 |
831 112 |
832 500 |
3,8 |
795 177 |
796 738 |
798 524 |
799 530 |
800 865 |
| DC45 |
265 481 |
270 158 |
274 657 |
279 070 |
283 463 |
13,9 |
228 579 |
232 606 |
236 480 |
240 279 |
244 062 |
| DC47 |
1 216 451 |
1 227 904 |
1 239 350 |
1 249 787 |
1 261 291 |
5,6 |
1 148 330 |
1 159 141 |
1 169 946 |
1 179 799 |
1 190 659 |
| DC48 |
943 535 |
956 893 |
969 545 |
982 753 |
996 636 |
24,1 |
716 143 |
726 282 |
735 885 |
745 910 |
756 447 |
| EKU |
3 910 546 |
3 996 528 |
4 080 699 |
4 165 110 |
4 250 640 |
23,8 |
2 979 836 |
3 045 354 |
3 109 493 |
3 173 814 |
3 238 988 |
| ETH |
3 904 334 |
3 961 457 |
4 018 350 |
4 072 927 |
4 125 608 |
18,9 |
3 166 415 |
3 212 742 |
3 258 882 |
3 303 144 |
3 345 868 |
| JHB |
5 781 281 |
5 951 077 |
6 121 322 |
6 295 072 |
6 465 812 |
22,2 |
4 497 837 |
4 629 938 |
4 762 389 |
4 897 566 |
5 030 402 |
| MAN |
861 046 |
869 265 |
877 233 |
884 908 |
892 675 |
20,0 |
688 837 |
695 412 |
701 786 |
707 926 |
714 140 |
| NMA |
1 208 262 |
1 211 496 |
1 214 323 |
1 216 179 |
1 218 016 |
20,4 |
961 777 |
964 351 |
966 601 |
968 078 |
969 541 |
| TSH |
3 672 841 |
3 767 270 |
3 860 013 |
3 950 218 |
4 038 360 |
30,6 |
2 548 952 |
2 614 485 |
2 678 849 |
2 741 451 |
2 802 622 |
2. Socio-economic and environmental risk factors
As expected, COVID-19 exacerbated pre-existing poverty and inequalities on a global scale. As much as it was a health crisis, it also disrupted livelihoods and exposed societal weaknesses, which ultimately intensified the impact of the pandemic. As one of the most unequal countries in the world, South Africa experienced a widening gap between the rich and the poor during the pandemic. The poor were hardest hit after many lost their jobs and had their income reduced. From an economic perspective, the pandemic led to a sharp 7% decline in the country’s Gross Domestic Product (GDP) in 2020, and a rise in unemployment rates. When comparing unemployment rates in the fourth quarters of the period from 2020 to 2022, unemployment was highest in 2021 at 35.3%. Unemployment does appear to be easing, as total employment increased by 1.4 million people between the fourth quarters of 2021 and 2022.21
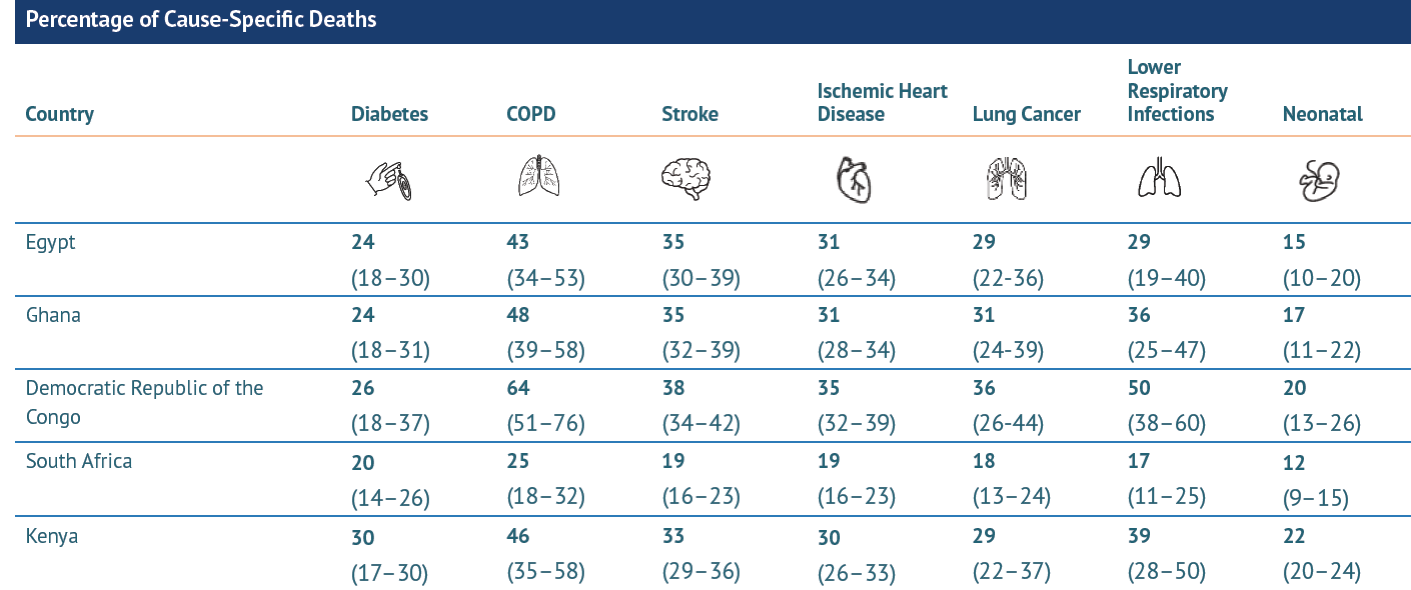
An interesting phenomenon of the COVID-19 lockdowns was how blue skies appeared in some of the world’s most polluted areas due to reduced industrial activity and fewer cars on the roads.22 This was a temporary fix, however, as air pollution continues to be one of the leading and most direct environmental threats to human health. Pollution is linked to increased susceptibility to respiratory infections, including COVID-19. Furthermore, long-term exposures to air pollution have been linked to increased risk of illness and death from chronic diseases such as stroke, lung cancer, ischaemic heart disease, chronic obstructive pulmonary disease (COPD), type 2 diabetes23,24 and even stillbirths.25 The State of Air Quality and Health Impacts in Africa report summarised data on air pollution exposures and associated health impacts in Africa using data from the Global Burden of Disease (GBD) project. South Africa has some of the highest levels of air pollution in the world, and was one of the five countries whose data were analysed in the report, in addition to Egypt, Ghana, Kenya and the Democratic Republic of Congo. The report estimated that in 2019, the death rate linked to household and ambient air pollution in South Africa was 44.6 (35.4-53.8) per 100 000 people per year. Figure 2 shows the percentage of cause-specific deaths linked to air pollution, with estimates being highest for COPD and diabetes in South Africa.23 The latest data from the Air Quality Life Index (AQLI) illustrates that permanently reducing global air pollution to meet the WHO’s guideline would add 2.2 years onto average life expectancy globally, and 1.5 years for South Africa specifically. However, in order for that to happen, strategies that reduce exposure and vulnerability to air pollution need to be developed to reduce the burden on public health.22,24

Figure 2.Percentage of cause-specific deaths linked to air pollution in five focus countries in Africa, 2019
The 2021/22 Human Development Report developed a COVID-19-adjusted human development index (HDI) quantifying the complexity of the crisis from a multi-dimensional view.26 Interestingly, South Africa’s human development rank (HDR) improved from 115 in 2019 to 102 in 2020, while the HDI remained relatively constant in 2019 (0.736), 2020 (0.727), and 2021 (0.713), as illustrated in Table 5. The countries with the highest HDI ranking were Norway, Iceland and Switzerland. Coincidentally, these three countries were also ranked among the top 10 happiest in the world according to the 2023 World Happiness Report.27 South Africa was ranked 85th among 109 countries between 2020 and 2022. The happiness scores were determined based on six key variables: GDP per capita, social support, healthy life expectancy, freedom to make life choices, generosity, and freedom from corruption. One of the central findings of the report was that the quality of social context, particularly the extent to which people trusted the government and the extent to which they trusted the compassion of their peers, supported their happiness before and during the pandemic, and likely after the pandemic too.
Table 5.Socio-economic indicators by province, 2019-2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Age-standardized mortality rate attributed to household and ambient air pollution (per 100 000 population) |
2019 |
WHO |
74,9 |
|
|
|
|
|
|
|
|
|
a |
| WHO COPD |
5,2 |
|
|
|
|
|
|
|
|
|
a |
| WHO Ischeamic heart disease |
15,3 |
|
|
|
|
|
|
|
|
|
a |
| WHO Lower respiratory infections |
20,7 |
|
|
|
|
|
|
|
|
|
a |
| WHO Stroke |
10,2 |
|
|
|
|
|
|
|
|
|
a |
| WHO Trachea, bronchus, lung cancers |
2,9 |
|
|
|
|
|
|
|
|
|
a |
| SOGA |
44,6 |
|
|
|
|
|
|
|
|
|
b |
| Drinking Water System (Blue Drop) Performance Rating |
2021 |
Blue Drop Low risk |
48,0 |
51,9 |
37,7 |
82,8 |
48,0 |
35,6 |
58,9 |
46,7 |
12,2 |
85,0 |
c |
| |
Blue Drop Medium risk |
18,0 |
23,5 |
15,6 |
10,3 |
18,1 |
18,4 |
20,5 |
22,1 |
17,1 |
7,9 |
c |
| |
Blue Drop High risk |
11,0 |
11,2 |
19,5 |
3,4 |
7,4 |
21,8 |
8,0 |
11,6 |
17,7 |
3,1 |
c |
| |
Blue Drop Critical risk |
23,0 |
13,4 |
27,3 |
3,4 |
26,5 |
24,1 |
12,5 |
19,6 |
53,0 |
3,9 |
c |
| Education level: percentage of population with no schooling |
2021 |
both sexes 20 years and older GHS |
3,2 |
4,6 |
2,6 |
1,0 |
4,4 |
7,1 |
6,3 |
3,2 |
3,9 |
0,7 |
d |
| Human development index (high value = best) |
2019 |
both sexes all ages HDR |
0,71 |
|
|
|
|
|
|
|
|
|
e |
| 2020 |
both sexes all ages HDR |
0,73 |
|
|
|
|
|
|
|
|
|
f |
| 2021 |
both sexes all ages HDR |
0,7 |
|
|
|
|
|
|
|
|
|
f |
| Human development index rank (1= best) |
2019 |
both sexes all ages HDR |
115 |
|
|
|
|
|
|
|
|
|
e |
| 2020 |
both sexes all ages HDR |
102 |
|
|
|
|
|
|
|
|
|
f |
| Percentage of households by type of housing |
2021 |
both sexes GHS Formal |
83,6 |
72,4 |
82,6 |
81,6 |
85,7 |
96,3 |
89,8 |
86,8 |
80,5 |
82,2 |
d |
| |
both sexes GHS Informal |
11,7 |
5,4 |
15,4 |
17,0 |
5,0 |
2,9 |
7,1 |
12,3 |
19,1 |
17,3 |
d |
| |
both sexes GHS Traditional |
4,2 |
21,6 |
2,0 |
0,1 |
9,3 |
0,7 |
3,1 |
0,5 |
0,4 |
0,1 |
d |
| Percentage of households using electricity for cooking |
2021 |
GHS |
77,7 |
77,7 |
87,2 |
77,4 |
82,3 |
64,5 |
71,4 |
83,0 |
78,8 |
80,5 |
d |
| Percentage of households with access to improved sanitation |
2019 |
GHS |
82,1 |
87,6 |
82,3 |
90,0 |
80,9 |
63,4 |
63,7 |
83,9 |
68,8 |
94,5 |
g |
| 2020 |
GHS |
83,2 |
92,7 |
85,8 |
90,5 |
81,2 |
58,7 |
64,4 |
86,9 |
78,3 |
93,9 |
d |
| 2021 |
GHS |
84,1 |
91,7 |
86,3 |
91,8 |
84,5 |
58,5 |
63,2 |
87,4 |
77,8 |
94,8 |
d |
| Percentage of households with access to piped water |
2020 |
GHS |
89,1 |
72,1 |
93,3 |
98,0 |
86,9 |
71,3 |
87,9 |
91,8 |
87,3 |
98,5 |
d |
| 2021 |
GHS |
88,7 |
71,0 |
93,6 |
98,4 |
87,0 |
69,4 |
86,2 |
90,9 |
83,4 |
99,4 |
d |
| Percentage of households with telephone (telephone in dwelling or cell phone) |
2021 |
GHS |
97,8 |
97,4 |
98,0 |
98,4 |
96,7 |
95,4 |
98,9 |
97,6 |
99,2 |
98,5 |
d |
| Percentage of population with primary reliance on clean fuels |
2019 |
WHO |
86,0 |
|
|
|
|
|
|
|
|
|
h |
| 2020 |
WHO |
87,0 |
|
|
|
|
|
|
|
|
|
i |
| Unemployment rate (official definition) |
2020 Q4 |
both sexes 15-64 years LFS |
32,5 |
47,9 |
33,4 |
34,1 |
29,6 |
27,3 |
33,0 |
28,7 |
33,3 |
22,5 |
j |
| 2021 Q4 |
both sexes 15-64 years LFS |
35,3 |
45,0 |
36,7 |
36,6 |
32,4 |
33,9 |
39,7 |
25,0 |
33,8 |
28,0 |
k |
| 2022 Q4 |
both sexes 15-64 years LFS |
32,7 |
42,1 |
22,1 |
34,0 |
31,4 |
31,8 |
36,1 |
22,1 |
37,0 |
22,5 |
l |
| Air pollution level in cities (particulate matter [PM]) |
2020 |
AQLI PM2.5 |
20,3 |
|
|
|
|
|
|
|
|
|
m |
| Wastewater systems (Green Drop) Performance Rating |
2021 |
Green Drop |
37,0 |
51,0 |
26,0 |
68,0 |
68,0 |
29,0 |
49,0 |
41,0 |
30,0 |
84,0 |
n |
| |
Green Drop Critical risk |
39,0 |
39,0 |
67,0 |
15,0 |
14,0 |
78,0 |
43,0 |
76,0 |
69,0 |
11,0 |
n |
Reference notes
a Global Health Observatory.28
b SOGA Africa 2021.23
c Blue Drop 2022.29
d GHS 2021.18
e HDR 2020.30
f HDR 2022.26
g Stats SA GHS 2019.16
h World Health Statistics 2021.31
i World Health Statistics 2022.32
j Labour Force Survey Q4 2020.33
k Labour Force Survey Q4 2021.34
l Labour Force Survey Q4 2022.21
m Air Quality Life Index 2022.22
n Green Drop 2022.35
Definitions
- Drinking Water System (Blue Drop) Performance Rating [Percentage]: Composite score measuring compliance of water suppliers with water quality management requirements. Includes microbiological, chemical and physical compliance criteria.
- Education level: percentage of population with no schooling [Percentage]: Percentage of people in a given age group who have received a particular level of education.
- Human development index (high value = best) [Number]: The HDI is a summary measure of human development. It measures the average achievements in a country in three basic dimensions of human development:
- Human development index rank (1 = best) [Number]: Rank from 1 to end given to each country according to value of HDI.
- Percentage of households by type of housing [Percentage]: Percentage of households that are categorised as formal, informal, traditional or other.
- Percentage of households using electricity for cooking [Percentage]: Percentage of households using electricity as their main energy source for cooking.
- Percentage of households with access to improved sanitation [Percentage]: Percentage of households using improved sanitation facilities (including flush to piped sewer system, flush to septic tank, flush/pour flush to pit, flush/pour flush to elsewhere).
- Percentage of households with access to piped water [Percentage]: Includes households with piped water in dwelling, piped water inside yard or piped water on a community stand (<200m away or further).
- Percentage of households with telephone (telephone in dwelling or cell phone) [Percentage]: Percentage of households with a telephone in the dwelling or a cellular telephone.
- Percentage of population with primary reliance on clean fuels [Percentage]: Percentage of population with primary reliance on clean fuels.
- Unemployment rate (official definition) [Percentage]: The official definition of the unemployed is that they are those people within the economically active population (aged 15-65) who:
(a) did not have a job or business during the 7 days prior to the interview,
(b) want to work and are available to work within two weeks of the interview, and
(c) have taken active steps to look for work or to start some form of self-employment in the 4 weeks prior to the interview.
- Wastewater systems (Green Drop) Performance Rating [Percentage]: Composite score measuring compliance of wastewater management requirements.
In 2022, the Department of Water and Sanitation released the first Blue Drop Progress Report since 2015, reporting on the current status and risk trends of municipal potable water-treatment facilities.29 A total of 144 water service authorities, comprising 1 186 water-supply systems in South Africa, were assessed to calculate the Blue Drop Risk Rating (BDRR). Overall, the National BDRR profile for the country was summarised as follows:
-
48% of water-supply systems were found to be in the low-risk category,
-
18% were in the medium-risk category,
-
11% were in the high-risk category, and
-
23% were in the critical-risk category.
The Green Drop Report, which was also released in 2022, focused on the state of wastewater treatment plants.35 The report covered audits of 995 wastewater networks and treatment works, operated by 144 water-service authorities (850 systems), 12 Department of Public Works operations (115 systems), and five private- and state-owned organisations (30 systems). Only 23 systems scored 90% or more, with most rural municipalities struggling to score more than 50%. A total of 334 (39%) of the municipal wastewater systems were identified to be in a critical state in 2021. Overall, the assessed risk deteriorated between 2013 and 2021.
Safe and readily available water is important for public health as contaminated water and poor sanitation are linked to transmission of gastrointestinal diseases such as cholera. During COVID-19, access to clean water was considered critical in the prevention of transmission. Water assessments should be conducted more frequently to ensure that systems and strategies are in place to reduce the risk to the people supplied by these two critical systems.
3. Disability
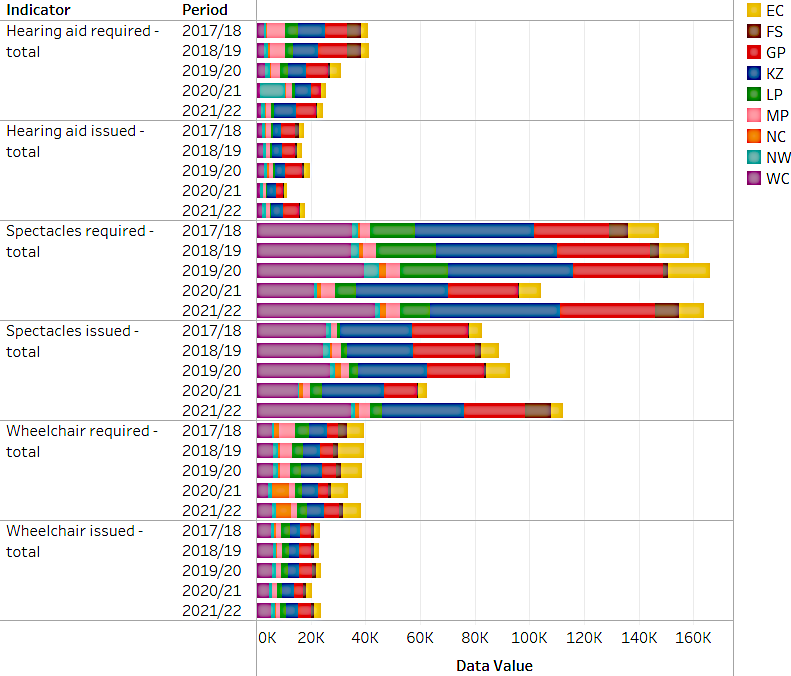
South Africans with disabilities were greatly and uniquely affected by COVID-19. They were at greater risk of poor outcomes from the disease; lockdown periods reduced their access to routine health care and rehabilitation services; and efforts to mitigate the pandemic led to adverse social impacts in this group.36 This situation was not unique to South Africa. The International Disability Alliance urged policy makers to make those living with disabilities a priority during the vaccination roll-out to prevent them from being left further behind, having to struggle with disproportionate loss of lives and livelihoods, inability to access healthcare services, and disconnection from the general population.37 In November 2022, the National Department of Women, Youth and Persons with Disabilities released a report on the impact of COVID-19 on persons with disabilities in South Africa, which stated that the rights of many persons with disabilities were either denied or limited during the pandemic, even though there were a few positive stories and experiences shared by some. With regard to health-related issues, the report highlighted that persons living with disabilities experienced difficulties with adhering to the mandatory COVID-19 guidelines such as social distancing and wearing of personal protective equipment (PPE), and accessing health care, therapy, medication, specialist care and assistive devices. Figure 3 shows that provision of assistive devices dropped substantially in 2020.38

Figure 3.Number of assistive devices required per province, 2017/18 - 2021/22
It has been found that people with disabilities are more likely to be older, female, poorer, and to have additional comorbidities than their able peers.36 As of 2021, more women were classified as disabled (4.9%) than men (4.1%).18 Living with disabilities leads to challenges in all aspects of life, including access to healthcare services, aids or devices, medication and support (for example, when caregivers are infected with COVID-19). These impacts are exacerbated in local and middle-income countries (LMICs), which often face additional challenges of corruption, political instability, lack of suitable transportation, and a general negative attitude to those living with disability, and to disability overall.39 Table 6 shows how the provision of assistive devices slowed down in 2020/21, particularly for spectacles. However, there was a steady improvement in the 2021/22 financial year, in some instances even returning to pre-pandemic levels.
Table 6.Disability indicators by province, 2019/20 - 2021/22
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Cataract surgery - total |
2019/20 |
both sexes all ages DHIS |
58 808 |
2 971 |
7 592 |
12 454 |
19 781 |
3 483 |
1 730 |
776 |
2 440 |
7 581 |
a |
|
2020/21 |
both sexes all ages DHIS |
19 108 |
362 |
313 |
4 339 |
9 660 |
1 427 |
|
601 |
166 |
2 240 |
a |
|
2021/22 |
both sexes all ages DHIS |
38 388 |
1 552 |
1 880 |
8 385 |
16 767 |
3 063 |
|
463 |
1 155 |
5 123 |
a |
| Cataract surgery rate |
2019/20 |
both sexes DHIS |
1 022,0 |
404,9 |
2 628,0 |
879,1 |
1 754,0 |
586,5 |
380,9 |
630,8 |
606,4 |
1 133,0 |
a |
|
2020/21 |
both sexes DHIS |
262,9 |
48,9 |
106,0 |
296,3 |
819,1 |
232,8 |
0,0 |
488,3 |
41,1 |
333,4 |
a |
|
2021/22 |
both sexes DHIS |
633,4 |
231,1 |
646,0 |
524,1 |
1 450,0 |
503,4 |
|
357,0 |
277,0 |
719,6 |
a |
| Hearing aid issued - total |
2019/20 |
both sexes all ages DHIS |
19 890 |
2 223 |
680 |
6 418 |
3 663 |
641 |
1 630 |
430 |
1 314 |
2 891 |
a |
|
2020/21 |
both sexes all ages DHIS |
11 489 |
1 281 |
270 |
2 794 |
3 102 |
373 |
1 041 |
164 |
916 |
1 548 |
a |
|
2021/22 |
both sexes all ages DHIS |
17 794 |
1 576 |
437 |
5 924 |
4 374 |
467 |
1 288 |
218 |
1 187 |
2 323 |
a |
| Hearing aid issued adult 19 years and older |
2020/21 |
both sexes DHIS |
9 531 |
1 093 |
160 |
2 463 |
2 433 |
293 |
941 |
118 |
722 |
1 308 |
a |
|
2021/22 |
both sexes DHIS |
14 481 |
1 222 |
251 |
5 130 |
3 249 |
376 |
1 107 |
155 |
1 042 |
1 949 |
a |
| Hearing aid issued adult 19 years and older rate |
2020/21 |
both sexes DHIS |
41,9 |
72,2 |
124,0 |
80,9 |
47,6 |
36,9 |
42,6 |
52,0 |
8,6 |
99,2 |
a |
|
2021/22 |
both sexes DHIS |
71,2 |
71,4 |
137,2 |
78,5 |
53,5 |
31,4 |
68,1 |
54,0 |
103,4 |
113,8 |
a |
| Hearing aid issued child 0-18 years |
2020/21 |
both sexes DHIS |
1 958 |
188 |
110 |
331 |
669 |
80 |
100 |
46 |
194 |
240 |
a |
|
2021/22 |
both sexes DHIS |
3 313 |
354 |
186 |
794 |
1 125 |
91 |
181 |
63 |
145 |
374 |
a |
| Hearing aid issued child 0-18 years rate |
2020/21 |
both sexes DHIS |
66,8 |
53,6 |
323,5 |
73,9 |
76,7 |
58,8 |
45,7 |
107,0 |
37,0 |
79,2 |
a |
|
2021/22 |
both sexes DHIS |
77,6 |
64,8 |
357,7 |
79,3 |
63,1 |
51,7 |
88,7 |
76,8 |
109,8 |
127,6 |
a |
| Hearing aid required - total |
2019/20 |
both sexes all ages DHIS |
30 943 |
3 754 |
730 |
7 988 |
6 827 |
2 884 |
3 301 |
432 |
1 715 |
3 312 |
a |
|
2020/21 |
both sexes DHIS |
25 672 |
1 864 |
163 |
3 493 |
5 985 |
931 |
2 429 |
270 |
8 915 |
1 622 |
a |
|
2021/22 |
both sexes all ages DHIS |
24 606 |
2 258 |
235 |
7 538 |
7 860 |
1 372 |
1 829 |
369 |
1 140 |
2 005 |
a |
| Hearing aid required adult 19 years and older |
2020/21 |
both sexes DHIS |
22 741 |
1 513 |
129 |
3 045 |
5 113 |
795 |
2 210 |
227 |
8 390 |
1 319 |
a |
|
2021/22 |
both sexes DHIS |
20 338 |
1 712 |
183 |
6 537 |
6 078 |
1 196 |
1 625 |
287 |
1 008 |
1 712 |
a |
| Hearing aid required child 0-18 years |
2020/21 |
both sexes DHIS |
2 931 |
351 |
34 |
448 |
872 |
136 |
219 |
43 |
525 |
303 |
a |
|
2021/22 |
both sexes DHIS |
4 268 |
546 |
52 |
1 001 |
1 782 |
176 |
204 |
82 |
132 |
293 |
a |
| Hearing aids issued rate |
2019/20 |
both sexes all ages DHIS |
64,3 |
59,2 |
93,2 |
80,3 |
53,7 |
22,2 |
49,4 |
99,5 |
76,6 |
87,3 |
a |
|
2020/21 |
both sexes DHIS |
44,8 |
68,7 |
165,6 |
80,0 |
51,8 |
40,1 |
42,9 |
60,7 |
10,3 |
95,4 |
a |
|
2021/22 |
both sexes DHIS |
72,3 |
69,8 |
186,0 |
78,6 |
55,6 |
34,0 |
70,4 |
59,1 |
104,1 |
115,9 |
a |
| Prevalence of disability |
2021 |
both sexes 5+ years GHS |
4,5 |
4,8 |
4,9 |
3,1 |
5,5 |
5,2 |
3,8 |
7,1 |
4,6 |
4,9 |
b |
|
|
female 5+ years GHS |
4,9 |
|
|
|
|
|
|
|
|
|
b |
|
|
male 5+ years GHS |
4,1 |
|
|
|
|
|
|
|
|
|
b |
| Spectacles issued - total |
2019/20 |
both sexes all ages DHIS |
93 086 |
8 964 |
727 |
20 818 |
25 229 |
3 179 |
3 247 |
1 852 |
2 077 |
26 993 |
a |
|
2020/21 |
both sexes all ages DHIS |
62 739 |
3 500 |
394 |
11 845 |
23 026 |
4 363 |
2 547 |
1 201 |
395 |
15 468 |
a |
|
2021/22 |
both sexes all ages DHIS |
112 249 |
4 206 |
9 573 |
22 339 |
29 958 |
4 462 |
3 970 |
1 413 |
1 710 |
34 618 |
a |
| Spectacles issued rate |
2019/20 |
both sexes all ages DHIS |
56,0 |
57,3 |
44,3 |
63,0 |
55,4 |
18,2 |
63,7 |
65,6 |
38,6 |
68,3 |
a |
|
2020/21 |
both sexes all ages DHIS |
60,2 |
44,5 |
61,8 |
46,3 |
68,7 |
55,4 |
52,7 |
73,3 |
46,1 |
72,3 |
a |
|
2021/22 |
both sexes all ages DHIS |
68,5 |
46,8 |
109,1 |
64,3 |
62,7 |
40,7 |
77,3 |
67,9 |
98,2 |
79,2 |
a |
| Spectacles issued to an adult - total |
2020/21 |
both sexes DHIS |
56 913 |
3 340 |
361 |
10 561 |
19 652 |
4 034 |
2 334 |
1 173 |
374 |
15 084 |
a |
|
2021/22 |
both sexes DHIS |
98 553 |
3 844 |
9 172 |
18 934 |
25 338 |
3 968 |
3 311 |
1 357 |
1 522 |
31 107 |
a |
| Spectacles issued to an adult rate |
2020/21 |
both sexes DHIS |
61,5 |
56,3 |
71,8 |
44,7 |
70,7 |
56,9 |
50,9 |
74,0 |
49,1 |
73,0 |
a |
|
2021/22 |
both sexes DHIS |
69,9 |
49,3 |
134,8 |
65,6 |
63,1 |
41,5 |
78,8 |
67,6 |
98,0 |
77,7 |
a |
| Spectacles issued to child - total |
2020/21 |
both sexes DHIS |
5 826 |
160 |
33 |
1 284 |
3 374 |
329 |
213 |
28 |
21 |
384 |
a |
|
2021/22 |
both sexes DHIS |
13 696 |
362 |
401 |
3 405 |
4 620 |
494 |
659 |
56 |
188 |
3 511 |
a |
| Spectacles issued to child rate |
2020/21 |
both sexes DHIS |
49,7 |
8,3 |
24,4 |
64,6 |
58,8 |
41,4 |
84,2 |
52,8 |
22,1 |
51,8 |
a |
|
2021/22 |
both sexes DHIS |
59,6 |
30,4 |
20,3 |
57,8 |
60,4 |
35,1 |
70,6 |
76,7 |
99,5 |
95,9 |
a |
| Spectacles required - total |
2019/20 |
both sexes all ages DHIS |
166 220 |
15 637 |
1 641 |
33 068 |
45 567 |
17 467 |
5 101 |
2 823 |
5 379 |
39 537 |
a |
|
2020/21 |
both sexes all ages DHIS |
104 250 |
7 869 |
638 |
25 611 |
33 518 |
7 882 |
4 837 |
1 638 |
857 |
21 400 |
a |
|
2021/22 |
both sexes all ages DHIS |
163 908 |
8 980 |
8 778 |
34 741 |
47 778 |
10 965 |
5 137 |
2 080 |
1 742 |
43 707 |
a |
| Spectacles required by an adult - total |
2020/21 |
both sexes DHIS |
92 518 |
5 932 |
503 |
23 622 |
27 784 |
7 088 |
4 584 |
1 585 |
762 |
20 658 |
a |
|
2021/22 |
both sexes DHIS |
140 935 |
7 790 |
6 806 |
28 845 |
40 128 |
9 557 |
4 203 |
2 007 |
1 553 |
40 046 |
a |
| Spectacles required by child - total |
2020/21 |
both sexes DHIS |
11 732 |
1 937 |
135 |
1 989 |
5 734 |
794 |
253 |
53 |
95 |
742 |
a |
|
2021/22 |
both sexes DHIS |
22 973 |
1 190 |
1 972 |
5 896 |
7 650 |
1 408 |
934 |
73 |
189 |
3 661 |
a |
| Wheelchair issued - total |
2019/20 |
both sexes all ages DHIS |
23 611 |
1 792 |
1 271 |
4 643 |
4 155 |
2 614 |
1 720 |
241 |
1 183 |
5 992 |
a |
|
2020/21 |
both sexes all ages DHIS |
20 646 |
2 351 |
1 123 |
3 149 |
4 346 |
2 041 |
1 776 |
56 |
1 066 |
4 738 |
a |
|
2021/22 |
both sexes all ages DHIS |
23 653 |
2 298 |
1 242 |
4 706 |
4 537 |
2 076 |
1 651 |
309 |
1 176 |
5 658 |
a |
| Wheelchair issued adult 19 years and older |
2020/21 |
both sexes DHIS |
18 035 |
2 031 |
905 |
2 758 |
3 710 |
1 826 |
1 543 |
45 |
953 |
4 264 |
a |
|
2021/22 |
both sexes DHIS |
19 956 |
1 719 |
1 029 |
4 066 |
3 676 |
1 872 |
1 374 |
246 |
1 025 |
4 949 |
a |
| Wheelchair issued adult 19 years and older rate |
2020/21 |
both sexes DHIS |
62,10 |
39,10 |
87,40 |
91,50 |
76,90 |
81,30 |
94,40 |
0,81 |
65,60 |
104,00 |
a |
|
2021/22 |
both sexes DHIS |
61,50 |
31,30 |
88,60 |
86,80 |
73,00 |
62,10 |
78,90 |
5,00 |
72,90 |
99,90 |
a |
| Wheelchair issued child 0-18 years |
2020/21 |
both sexes DHIS |
2 611 |
320 |
218 |
391 |
636 |
215 |
233 |
11 |
113 |
474 |
a |
|
2021/22 |
both sexes DHIS |
3 697 |
579 |
213 |
640 |
861 |
204 |
277 |
63 |
151 |
709 |
a |
| Wheelchair issued child 0-18 years rate |
2020/21 |
both sexes DHIS |
58,9 |
41,9 |
137,1 |
74,5 |
52,2 |
86,0 |
54,8 |
1,8 |
87,6 |
136,2 |
a |
|
2021/22 |
both sexes DHIS |
62,5 |
62,1 |
61,7 |
70,0 |
67,2 |
54,3 |
66,0 |
11,6 |
101,3 |
74,6 |
a |
| Wheelchair required - total |
2019/20 |
both sexes all ages DHIS |
38 898 |
7 725 |
1 763 |
5 288 |
7 777 |
3 945 |
3 590 |
626 |
1 855 |
6 329 |
a |
|
2020/21 |
both sexes DHIS |
33 485 |
5 957 |
1 195 |
3 539 |
6 043 |
2 496 |
2 060 |
6 167 |
1 581 |
4 447 |
a |
|
2021/22 |
both sexes all ages DHIS |
38 366 |
6 433 |
1 506 |
5 599 |
6 318 |
3 389 |
2 162 |
5 502 |
1 555 |
5 902 |
a |
| Wheelchair required adult 19 years and older |
2020/21 |
both sexes DHIS |
29 052 |
5 193 |
1 036 |
3 014 |
4 825 |
2 246 |
1 635 |
5 552 |
1 452 |
4 099 |
a |
|
2021/22 |
both sexes DHIS |
32 452 |
5 500 |
1 161 |
4 685 |
5 036 |
3 013 |
1 742 |
4 957 |
1 406 |
4 952 |
a |
| Wheelchair required child 0-18 years |
2020/21 |
both sexes DHIS |
4 433 |
764 |
159 |
525 |
1 218 |
250 |
425 |
615 |
129 |
348 |
a |
|
2021/22 |
both sexes DHIS |
5 914 |
933 |
345 |
914 |
1 282 |
376 |
420 |
545 |
149 |
950 |
a |
| Wheelchairs issued rate |
2019/20 |
both sexes all ages DHIS |
60,7 |
23,2 |
72,1 |
87,8 |
53,4 |
66,3 |
47,9 |
38,5 |
63,8 |
94,7 |
a |
|
2020/21 |
both sexes DHIS |
61,7 |
39,5 |
94,0 |
89,0 |
71,9 |
81,8 |
86,2 |
0,9 |
67,4 |
106,5 |
a |
| |
2021/22 |
both sexes DHIS |
61,7 |
35,7 |
82,5 |
84,1 |
71,8 |
61,3 |
76,4 |
5,6 |
75,6 |
95,9 |
a |
Reference notes
a webDHIS.10
b GHS 2021.18
Definitions
- Cataract surgery - total [Number]: Number of eyes on which cataract surgery was performed.
- Hearing aid issued - total [Number]: All hearing aids issued to patients.
- Hearing aid issued adult 19 years and older [Number]: All hearing aids issued to adults 19 years and older.
- Hearing aid issued child 0-18 years [Number]: All hearing aids issued to children 0 to 18 years.
- Hearing aid required - total [Number]: All hearing aids required.
- Hearing aid required adult 19 years and older [Number]: All hearing aids required by adults 19 years and older.
- Hearing aid required child 0-18 years [Number]: All hearing aids required by children 0-18 years.
- Spectacles issued - total [Number]: Number of spectacles issued to patients.
- Spectacles issued to an adult - total [Number]: Number of spectacles issued to clients aged 19 years and older.
- Spectacles issued to child - total [Number]: Number of spectacles issued to clients aged 7-18 years of age.
- Spectacles required - total [Number]: Number of new spectacles (ordered) required for clients.
- Spectacles required by an adult - total [Number]: Spectacles (ordered) required for clients aged 19 years and above.
- Spectacles required by child - total [Number]: Spectacles (ordered) required for clients aged 7-18 years of age.
- Wheelchairs issued - total [Number]: All wheelchairs issued to a client in need of a wheelchair.
- Wheelchair issued adult 19 years and older [Number]: All wheelchairs issued to adults 19 years and older
- Wheelchair issued child 0-18 years [Number]: All wheelchairs issued to children 0-18 years.
- Wheelchair required - total [Number]: All wheelchair requests received at the facility.
- Wheelchair required adult 19 years and older [Number]: All wheelchair requests received at the facility for adults 19 years and older.
- Wheelchair required child 0-18 years [Number]: All wheelchair requests received at the facility for children 0-18 years.
- Cataract surgery rate [per 1 million]: Clients who had cataract surgery per 1 million uninsured population.
- Hearing aid issued adult 19 years and older rate [Percentage]: Hearing aids issued as a proportion of the applications for hearing aids received for adults 19 years and older.
- Hearing aid issued child 0-18 years rate [Percentage]: Hearing aids issued as a proportion of the applications for hearing aids received for children 0-18 years.
- Hearing aids issued rate [Percentage]: Hearing aids issued as a proportion of the applications for hearing aids received.
- Prevalence of disability [Percentage]: Percentage of people reporting moderate to severe disability in a survey where disability is defined as a limitation in one or more activities of daily living (seeing, hearing, communication, moving, getting around, daily life activities, learning, intellectual and emotional).
- Spectacles issued rate [Percentage]: Spectacles issued as a % of the applications received.
- Spectacles issued to an adult rate [Percentage]: Spectacles issued to adults aged 19 years and above as a proportion of the applications received in adults aged 19 years and above (required).
- Spectacles issued to child rate [Percentage]: Spectacles issued to children age 7-18 years as a proportion of the applications received in children 7-18 years of age (required).
- Wheelchair issued adult 19 years and older rate [Percentage]: Wheelchairs issued as a proportion of the applications for wheelchairs received for adults 19 years and older.
- Wheelchair issued child 0-18 years rate [Percentage]: Wheelchairs issued as a proportion of the applications for wheelchairs received for children 0-18 years.
- Wheelchairs issued rate [Percentage]: Wheelchairs issued as a proportion of the applications for wheelchairs received.
The COVID-19 pandemic has highlighted the need for strategies to better reach the 15% of the population living with disabilities worldwide.36
4. Nutrition
The COVID-19 pandemic had various impacts on nutrition globally, ranging from disruptions in food-supply chains and decreased food security and affordability, to increased risk of obesity, and changes in eating habits and breastfeeding of babies.40
COVID-19 had a significant impact on the ability of mothers to breastfeed their babies due to fears of transmission.41 This led to a reduction in breastfeeding rates, as shown in Table 7, and an increased risk of malnutrition in infants. This reduction in breastfeeding appears to be persisting in South Africa across most provinces, except for Gauteng and the Western Cape where the rates of exclusive breastfeeding in infants remained fairly stable.
Table 7.Nutrition indicators by province, 2019-2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
Infant exclusively breastfed at
DTaP-IPV-Hib-HBV 3rd dose rate |
2019/20 |
both sexes DHIS |
48,8 |
48,2 |
53,6 |
45,7 |
56,5 |
40,3 |
51,9 |
55,9 |
59,7 |
39,7 |
a |
| 2020/21 |
both sexes DHIS |
45,9 |
45,2 |
46,4 |
45,2 |
56,7 |
38,1 |
43,0 |
52,7 |
41,6 |
37,6 |
a |
| 2021/22 |
both sexes DHIS |
44,4 |
43,2 |
43,8 |
46,7 |
56,3 |
32,7 |
38,8 |
49,0 |
33,2 |
40,3 |
a |
| Overweight |
2020 |
both sexes Under
5 years WHO |
12,9 |
|
|
|
|
|
|
|
|
|
b |
| Stunting |
2020 |
both sexes WHO |
23,2 |
|
|
|
|
|
|
|
|
|
b |
| Vitamin A dose 12-59 months |
2019/20 |
both sexes DHIS |
5 302 353 |
772 904 |
226 520 |
1 067 632 |
1 455 506 |
496 909 |
466 125 |
80 536 |
265 752 |
470 469 |
a |
| 2020/21 |
both sexes DHIS |
3 898 515 |
540 386 |
198 276 |
850 985 |
898 699 |
409 577 |
345 116 |
69 451 |
209 734 |
376 291 |
a |
| 2021/22 |
both sexes DHIS |
4 428 184 |
577 730 |
203 706 |
982 671 |
1 030 246 |
439 413 |
400 232 |
73 845 |
271 654 |
448 687 |
a |
| Vitamin A dose 12-59 months coverage |
2019/20 |
both sexes DHIS |
56,6 |
58,1 |
52,1 |
52,7 |
68,2 |
46,5 |
65,6 |
48,4 |
41,6 |
53,9 |
a |
| 2020/21 |
both sexes DHIS |
49,5 |
49,1 |
48,1 |
47,4 |
60,6 |
43,6 |
51,1 |
47,6 |
37,9 |
44,0 |
a |
| 2021/22 |
both sexes DHIS |
60,3 |
63,7 |
55,7 |
57,1 |
78,2 |
49,5 |
57,9 |
42,5 |
50,9 |
51,4 |
a |
Reference notes
a webDHIS.10
b World Health Statistics 2022.32
Definitions
- Vitamin A dose 12-59 months [Number]: Vitamin A dose given to a child, preferably every six months from 12 to 59 months.
- Infant exclusively breastfed at DTaP-IPV-Hib-HBV 3rd dose rate [Percentage]: Infants exclusively breastfed at 14 weeks as a proportion of the DTaP-IPV-Hib-HBV 3rd dose vaccination. Take note that DTaP-IPV-Hib-HBV 3rd dose (Hexavalent) was implemented in 2015 to include the HepB dose.
- Obesity [Percentage]: Percentage of people with a body mass index (BMI) (body mass in kg divided by the square of the height in m) equal to or more than 30kg/m2.
- Overweight [Percentage]: Children: Proportion of children with weight for height over 2 standard deviations from the norm (reference population median). Adults: Percentage of people with body mass index (BMI) of 25-29.9 kg/m2. BMI is weight in kg divided by the square of height in m.
- Stunting [Percentage]: Proportion of children with height for age under 2 standard deviations from the norm (reference population median).
- Vitamin A dose 12-59 months coverage [Percentage]: Proportion of children 12-59 months who received vitamin A 200 000 units, preferably every six months. The denominator is therefore the target population 1-4 years multiplied by 2.
Vitamin A is vital to child health and immune function and programmes to control vitamin A deficiency contribute to a child’s chances of survival, reduce severity of childhood illnesses, and lead to overall reduction in child morbidity and mortality.42 As such, it was alarming to note the huge reduction in vitamin A doses administered in the country between 2019/20 and 2020/21, from 5.3 million to 3.9 million (Table 7). Administration of vitamin A has recovered somewhat, with the vitamin A dose coverage having increased from a low of 49.5% in 2020/21 to 60.3% 2021/22.
5. Health status indicators
5.1. Mortality
The 2022 edition of the World Health Organization’s World Health Statistics included an estimate of global mortality attributable to COVID-19, as of 20 April of that year.32 The WHO noted that although available data pointed to more than 4.7 million of the total of 6.2 million reported deaths having occurred in the Americas and European regions, mortality data in many countries were incomplete. One significant statistic, which was widely reported, was the estimate of excess mortality, which is defined as “the difference in the total number of deaths in a crisis compared to those expected under normal conditions”. Between January 2020 and December 2021, the full death toll associated directly and indirectly with the COVID-19 pandemic was approximately 14.9 million, exceeding the 5.4 million COVID-19 deaths by 9.5 million. Of these, 4.5 million excess deaths were estimated to have occurred in 2020, the balance of 10.4 million in 2021. The WHO pointed out that 10 countries, in which 35% of the global population resided, accounted for almost 70% of excess deaths worldwide. More than half of the excess deaths (53%) were estimated to have occurred in lower-middle-income countries, and more than a quarter (28%) in upper-middle-income countries. An attempt to estimate excess deaths, taking into account countries with incomplete data, came to a figure of 14.83 million excess deaths globally in the same 24-month period.43
In South Africa, the excess death reports44 generated by the South African Medical Research Council (SAMRC) were watched closely. Figure 4 and Table 8 show that a total of 339 146 excess deaths were estimated between May 2020 and December 2022. The close correlation between excess deaths and the first four ‘waves’ of COVID-19 is immediately evident, as is the more diffuse picture associated with the Omicron variant in 2022. The weekly excess-deaths reports were discontinued after December 2022. The SAMRC now reports on weekly number of deaths in South Africa on a monthly basis, the most recent being for February 2023. The revised reporting is only at national level, disaggregated by age groups and natural and unnatural causes.
_in_south_africa__29_december_2019_-_10_december_2022.png)
Figure 4.Weekly deaths (all causes) in South Africa, 29 December 2019 - 10 December 2022
Table 8.Number of excess natural deaths by province relative to revised predicted numbers, 2022
| Region |
Period |
Excess deaths vs base |
Excess deaths per 100 000 population |
Age standardised excess deaths per 100 000 |
| South Africa |
3 May 20 - 10 Dec 22 |
33 9146 |
570 |
570 |
| Eastern Cape |
31 May 20 - 10 Dec 22 |
59 139 |
899 |
724 |
| Free State |
21 Jun 20 - 10 Dec 22 |
19 502 |
670 |
670 |
| Gauteng |
7 Jun 20 - 10 Dec 22 |
66 564 |
427 |
469 |
| KwaZulu-Natal |
7 Jun 20 - 10 Dec 22 |
70 009 |
612 |
704 |
| Limpopo |
21 Jun 20 - 10 Dec 22 |
37 990 |
643 |
563 |
| Mpumalanga |
21 Jun 20 - 10 Dec 22 |
26 013 |
541 |
583 |
| Northern Cape |
28 Jun 20 - 10 Dec 22 |
10 338 |
883 |
826 |
| North West |
28 Jun 20 - 10 Dec 22 |
18 330 |
455 |
467 |
| Western Cape |
3 May 20 - 10 Dec 22 |
31 260 |
443 |
390 |
Table 9 shows the life expectancy at birth for both sexes had dropped from 65.4 years in 2020 to 62 years in South Africa at the height of the COVID-19 pandemic in 2021. However, there was a slight recovery in 2022 and it increased to 62.8 for both sexes according to the Statistics South Africa mid-year population estimates.
Table 9.Mortality indicators by province, 2018 - 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
Adult mortality (45q15 - probability
of dying between 15-60 years of age) |
2018 |
both sexes RMS |
31,0 |
|
|
|
|
|
|
|
|
|
a |
| female RMS |
25,0 |
|
|
|
|
|
|
|
|
|
a |
| male RMS |
37,0 |
|
|
|
|
|
|
|
|
|
a |
| 2019 |
both sexes RMS |
29,0 |
|
|
|
|
|
|
|
|
|
b |
| female RMS |
24,0 |
|
|
|
|
|
|
|
|
|
b |
| male RMS |
35,0 |
|
|
|
|
|
|
|
|
|
b |
| 2020 |
both sexes RMS |
31,0 |
|
|
|
|
|
|
|
|
|
b |
| female RMS |
26,0 |
|
|
|
|
|
|
|
|
|
b |
| male RMS |
36,0 |
|
|
|
|
|
|
|
|
|
b |
| Healthy life expectancy (HALE) |
2019 |
both sexes WHO |
56,2 |
|
|
|
|
|
|
|
|
|
c |
| 56,2 |
|
|
|
|
|
|
|
|
|
d |
| female WHO |
57,7 |
|
|
|
|
|
|
|
|
|
c |
| 57,7 |
|
|
|
|
|
|
|
|
|
d |
| male WHO |
54,6 |
|
|
|
|
|
|
|
|
|
c |
| 54,6 |
|
|
|
|
|
|
|
|
|
d |
| Life expectancy at birth |
2020 |
both sexes mid-year |
65,4 |
|
|
|
|
|
|
|
|
|
e |
| both sexes RMS |
64,7 |
|
|
|
|
|
|
|
|
|
b |
| female mid-year |
68,5 |
|
|
|
|
|
|
|
|
|
f |
| female mid-year without HIV/AIDS |
71,3 |
|
|
|
|
|
|
|
|
|
f |
| female RMS |
67,2 |
|
|
|
|
|
|
|
|
|
b |
| female UNICEF |
68,0 |
|
|
|
|
|
|
|
|
|
g |
| male mid-year |
62,5 |
|
|
|
|
|
|
|
|
|
f |
| male mid-year without HIV/AIDS |
64,6 |
|
|
|
|
|
|
|
|
|
f |
| male RMS |
62,2 |
|
|
|
|
|
|
|
|
|
b |
| 2021 |
HDR |
62,3 |
|
|
|
|
|
|
|
|
|
h |
| both sexes mid-year |
62,0 |
|
|
|
|
|
|
|
|
|
i |
| female mid-year |
64,6 |
|
|
|
|
|
|
|
|
|
i |
| male mid-year |
59,3 |
|
|
|
|
|
|
|
|
|
i |
| 2022 |
both sexes mid-year |
62,8 |
|
|
|
|
|
|
|
|
|
e |
| female mid-year |
65,6 |
|
|
|
|
|
|
|
|
|
e |
| male mid-year |
60,0 |
|
|
|
|
|
|
|
|
|
e |
Reference notes
a RMS 2018.45
b RMS 2019 & 2021.46
c World Health Statistics 2021.31
d World Health Statistics 2022.32
e Stats SA MYE 2022.11
f Stats SA MYE 2020.13
g SWChildren 2021.47
h HDR 2022.26
i Stats SA MYE 2021.12
Definitions
- Adult mortality (45q15 - probability of dying between 15-60 years of age) [Percentage]: The probability of dying between 15 and 60 years of age (percentage of 15-year-olds who die before their 60th birthday).
- Healthy life expectancy (HALE) [Years]: Healthy life expectancy or health-adjusted life expectancy is based on life expectancy at birth but includes an adjustment for time spent in poor health. It is most easily understood as the equivalent number of years in full health that a newborn can expect to live based on current rates of ill-health and mortality.
- Life expectancy at birth [Years]: The average number of additional years a person could expect to live if current mortality trends were to continue for the rest of that person’s life.
5.2. Infectious diseases
Despite the impact of COVID-19, the number of malaria cases and deaths remained stable across the world without any major setbacks in malaria testing, prevention, and treatment services as countries intensified their efforts in their fight against malaria.48 Globally, the 2022 World Malaria report reported an estimated 619 000 deaths in 2021 compared to 625 000 in 2020 when the pandemic first hit, and 568 000 deaths pre-pandemic in 2019. Although the number of malaria cases continued to rise between 2020 and 2021, they rose at a slower rate than between 2019 and 2020. When looking at cases and deaths in the WHO African Region (Figure 5), which accounted for 95% of cases and 96% of deaths globally, there is an evident spike in both incidence and mortality rates in 2020, with reductions in both measures in 2021.

Figure 5.Malaria case incidence and mortality rates in the WHO African region, 2000-2021
South Africa was one of the countries that continued to make progress towards the elimination of malaria by 2025, with a 33.7% reduction in cases in 2021 compared to 2020. However, these figures could have been confounded by the reduction in testing due to limited movement during the lockdown periods when mobile clinics were unable to carry out testing and case investigations at community level. Furthermore, the country also recorded the highest increase in unclassified cases (one-third of total cases) over the past three years.48 A total of 4 109 malaria cases and 34 malaria deaths (Table 10) were reported by the National Department of Health (NDoH) from January 2022 to October 2022. In South Africa, malaria is classified as a category one Notifiable Medical Condition (MNC) that must be reported within 24 hours of diagnosis via written or electronic communication.49
At the beginning of 2022, the WHO and United Nations International Children’s Emergency Fund (UNICEF) reported an alarming increase in measles cases worldwide, with a 79% increase in the first two months of 2022 compared to the same period in the previous year. Health officials linked this surge in measles with the drop in vaccinations after the pandemic, as 23 million children missed out on all basic vaccinations in 2020. This represents the highest number of missed doses since 2009. COVID-19 disrupted childhood vaccinations as parents were apprehensive about taking their children to health facilities for fear of exposing them to COVID-19, and healthcare workers were reassigned to manage COVID-19 and moved away from doing routine vaccinations.50
South Africa also experienced a measles outbreak in October 2022. A total of 665 laboratory-confirmed measles cases were reported between 11 October 2022 and 24 February 2023 (Table 10) by the National Institute for Communicable Diseases (NICD). Although cases were reported across the country, outbreaks were declared in all provinces except the Eastern Cape. An outbreak is only declared once there are three or more classified laboratory measles cases reported within 30 days of onset of the disease. The most affected age groups were 5-9-year-olds (41% of cases), 1-4-year-olds (25% of cases) and 10-14-year-olds (20% of cases). In response to the outbreak, the NDoH initiated a national measles vaccination campaign for children aged between 6 months and 14 years, with the aim of limiting the outbreak. Health officials have been conducting vaccinations at schools, day-care centres and city clinics as part of the campaign to curb further spread of the outbreak.51
Table 10.Infectious disease indicators by province, 2018 - 2023
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Reported cases of malaria |
2020 |
both sexes all ages WHO |
4 463 |
|
|
|
|
|
|
|
|
|
a |
| 2021 |
both sexes all ages DOH surveillance |
4 300 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages WHO |
2 958 |
|
|
|
|
|
|
|
|
|
a |
| 2022 |
both sexes all ages DOH surveillance |
4 109 |
|
|
|
|
|
|
|
|
|
b |
| Reported cases of measles |
2018 |
WHO |
52,0 |
|
|
|
|
|
|
|
|
|
c |
| 2022/23 |
NICD lab diagnosed |
665 |
4 |
24 |
90 |
15 |
232 |
100 |
5 |
185 |
10 |
d |
| Reported deaths from malaria |
2020 |
both sexes all ages WHO |
38 |
|
|
|
|
|
|
|
|
|
a |
| 2021 |
both sexes all ages DOH surveillance |
49 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages WHO |
56 |
|
|
|
|
|
|
|
|
|
a |
| 2022 |
both sexes all ages DOH surveillance |
34 |
|
|
|
|
|
|
|
|
|
b |
Reference notes
a World Malaria 2022.48
b NICD Communique Dec 2022.49
c WHO Measles.28
d NICD Outbreak report 2023.52
5.3. Tuberculosis
Until the COVID-19 pandemic occurred, tuberculosis (TB) was one of the leading causes of death among the infectious diseases.53 According to the 2022 Global Tuberculosis Report, COVID-19 had a large impact on TB services globally.54 Worldwide, progress towards reducing TB disease burden slowed drastically, halted, and in some cases reversed, due to the pandemic.55 In South Africa, TB resources were redirected to address the demands posed by the pandemic.56 This redirection of resources affected the screening, diagnosis and treatment of TB, and slowed the progress made in the TB programme. South Africa is still among the five countries in the world with the highest TB incidence (Figure 6), although the situation has improved from 988 cases per 100 000 population per year in 2015 to 513/100 000 in 2021. South Africa is thus well on its way to reaching one of the 2025 End TB Milestones, namely a 50% reduction in TB incidence.57 However, the country needs to effectively implement the TB Recovery Plan, jointly developed by the National Department of Health and the TB Think Tank.55 Key to this effort is the concept of Targeted Universal Testing for TB (TUTT). Four key aims of the Plan are to reduce the number of undiagnosed people with TB, strengthen linkages to care, improve retention in care, and improve access to TB preventive treatment.
__2021.png)
Figure 6.WHO global TB incidence by region (per 100 000 population per year), 2021
Source: WHO Global Health Observatory28
According to WHO estimations,57 304 000 people in South Africa developed TB in 2021, of whom only 181 699 were diagnosed and started on treatment. TB-related deaths were estimated at 55 000 in 2021, with 33 000 of those having a TB/HIV co-infection due to the high double burden of HIV and TB in South Africa, and people living with HIV being at higher risk of contracting TB. Based on local routine monitoring (Table 11), the number of newly diagnosed drug-sensitive TB patients decreased from a peak of 222 569 pre-COVID (April 2019 - March 2020) to 158 764 (April 2020 - March 2021), which represented a (-29%) decline in new TB diagnosis, reversing the progress that had been made in the TB programme. The public health facilities heeded the call to action by integrating COVID-19 services and TB services, among other evidence-based interventions, which resulted in the number of new diagnoses growing in the following financial year, to 195 640 (April 2021 - March 2022). This represents an 84% recovery towards the 2019 financial year TB diagnosis and treatment numbers.
__2019_-_2022.png)
Table 11.TB diagnosis, year-on-year breakdown (provincial and national), 2019 - 2022
Table 11 provides a breakdown of declines per province, showing a decline in TB diagnosis and treatment in all provinces during the 2020/21 financial year and some recovery in TB diagnosis and treatment the following financial year. However, none of the provinces have managed to reach TB diagnosis and treatment numbers to the level prior to COVID-19 (April 2019 - March 2020).
Figure 7 (national) and Figure 8 (provincial) show the impact of COVID-19 and the subsequent lockdown conditions on TB screening. Slow recovery from the initial lockdown restrictions (depicted in red) can be observed, with TB screening numbers not making a full recovery to pre-COVID TB screening figures.
__jan.png)
Figure 7.Number of clients 5 years and older screened for TB symptoms in a facility (national), January 2020 - March 2022

Figure 8.Number of clients 5 years and older screened for TB in a facility by province, January 2020 - March 2022
The NDoH developed a National TB Recovery Plan58 with the aim of closing the gaps created by COVID-19, and leveraging good practices born from the response to COVID-19. Phase 1 (preparatory period) of the plan took place between January 2022 and June 2022, and Phase 2 (implementation period) began in July 2022 and ended in March 2023. The Plan outlined the following:
-
Finding undiagnosed people with TB through evidence-based interventions that scaled up community TB screening.55
-
The Targeted Universal TB Testing (TUTT) approach was strengthened. This offered, among other services, TB testing to people at high risk of contracting TB regardless of symptoms, as the National TB Prevalence Survey59 suggested that a large number of patients who develop TB present as asymptomatic.
-
Use of other technologies was scaled up, with a shorter turnaround time (TAT) for results compared to GeneXpert Ultra testing kits, which have a 48-hour TAT. These TB investigation tools will not replace GeneXpert Ultra testing, but will rather work alongside it. The TB diagnostic tools include, among others, the urine Lipoarabinomannan (LAM) screening (±25-minute TAT), digital X-rays (±20-minute TAT) and mobile self-screening applications. The latter proved to be effective in increasing COVID-19 screening coverage at a time of scarce human resources.
-
There was also an explicit effort to increase the focus on men, in response to the National TB Prevalence Survey59 which showed a higher prevalence of TB in males than females.
-
The recovery plan included strengthening of health systems that (i) support the TB programme, (ii) link people to TB care, and (iii) keep people in TB care through adherence counselling, hospital referrals to primary health care facilities, scale-up of shortened (6-month) multi-drug-resistant (MDR)-TB treatment regimens, 4-month paediatric treatment regimens for children, and strengthened tracer teams.
Figure 9 and Figure 10 show the impact of COVID-19 on TB diagnosis and treatment, with monthly data (24 months) displayed in relation to South African national lockdown levels from January 2020 to March 2022.
__january_2020_-_.png)
Figure 9.TB clients 5 years and older who started treatment in facility (national), January 2020 - March 2022

Figure 10.Drug-sensitive TB treatment started by persons 5 years and older, by province, January 2020 - March 2022
Drug-resistant (DR) TB was also negatively affected. There was a –32% decline in the number of people provided with treatment for rifampicin-resistant TB (RR-TB), while the number of people receiving MDR-TB treatment declined from 8 815 pre-COVID-19 to 6 016 in 2020/21, with a partial recovery to 7 005 (+16%) during 2021/22 (Table 12).
Table 12.TB indicators by province, 2019 - 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| All DS TB patients in cohort |
2019 |
both sexes DHIS |
220 171 |
42 453 |
10 994 |
31 394 |
51 296 |
10 601 |
12 146 |
7 215 |
13 153 |
40 919 |
a |
| 2020 |
both sexes DHIS |
165 624 |
32 873 |
7 803 |
22 310 |
37 584 |
8 204 |
8 979 |
5 616 |
9 748 |
32 507 |
a |
| 2021 |
both sexes DHIS |
121 883 |
25 561 |
5 569 |
15 658 |
27 188 |
5 190 |
6 007 |
4 119 |
6 945 |
25 646 |
a |
| Case detection rate (all forms) |
2020 |
both sexes Global TB |
58 |
|
|
|
|
|
|
|
|
|
b |
| 2021 |
both sexes Global TB |
57 |
|
|
|
|
|
|
|
|
|
b |
| DS TB patients who completed treatment or were cured |
2018 |
both sexes all ages DHIS |
174 583 |
30 909 |
8 633 |
27 955 |
41 577 |
9 221 |
10 479 |
3 720 |
7 553 |
34 536 |
a |
| 2019 |
both sexes DHIS |
176 032 |
33 474 |
8 520 |
26 340 |
42 449 |
8 289 |
9 823 |
5 409 |
10 334 |
31 394 |
a |
| 2020 |
both sexes DHIS |
130 598 |
25 697 |
5 824 |
18 387 |
31 184 |
6 377 |
7 233 |
3 844 |
7 708 |
24 344 |
a |
| Incidence of TB (all types) (per 100 000) |
2019 |
both sexes WHO |
615 |
|
|
|
|
|
|
|
|
|
c |
| 2020 |
both sexes WHO |
554 |
|
|
|
|
|
|
|
|
|
d |
| both sexes Global TB |
562 |
|
|
|
|
|
|
|
|
|
b |
| 2021 |
both sexes Global TB |
513 |
|
|
|
|
|
|
|
|
|
b |
| Screen for TB symptoms 5 years and older |
2019/20 |
both sexes DHIS |
88 341 637 |
11 911 051 |
4 997 501 |
17 309 676 |
23 697 914 |
10 873 851 |
6 544 049 |
1 569 752 |
4 881 165 |
6 556 678 |
a |
| 2020/21 |
both sexes DHIS |
70 565 171 |
9 493 199 |
3 546 481 |
14 079 732 |
19 132 526 |
9 023 591 |
5 270 205 |
1 236 609 |
3 752 773 |
5 030 055 |
a |
| 2021/22 |
both sexes DHIS |
80 942 655 |
10 532 623 |
3 607 012 |
17 268 185 |
21 143 838 |
9 727 357 |
6 018 633 |
1 593 266 |
4 385 597 |
6 666 144 |
a |
| Screen for TB symptoms under 5 years |
2019/20 |
both sexes DHIS |
17 647 545 |
2 154 997 |
926 337 |
3 204 481 |
4 514 276 |
2 584 786 |
1 547 206 |
291 499 |
938 084 |
1 485 879 |
a |
| 2020/21 |
both sexes DHIS |
13 189 701 |
1 715 142 |
650 304 |
2 468 495 |
3 384 940 |
1 876 971 |
1 137 773 |
219 538 |
657 298 |
1 079 240 |
a |
| 2021/22 |
both sexes DHIS |
15 632 660 |
1 977 308 |
716 311 |
3 010 670 |
3 776 483 |
2 231 014 |
1 386 491 |
286 590 |
834 127 |
1 413 666 |
a |
| TB child under 5 years start on treatment rate |
2019/20 |
DHIS |
11,3 |
9,6 |
4,5 |
15,0 |
11,1 |
7,6 |
3,5 |
11,6 |
10,1 |
40,7 |
a |
| 2020/21 |
DHIS |
93,2 |
99,5 |
103,7 |
80,0 |
92,4 |
62,9 |
122,3 |
70,1 |
108,7 |
99,2 |
a |
| 2021/22 |
DHIS |
94,8 |
79,6 |
65,6 |
98,7 |
101,8 |
105,7 |
87,6 |
114,4 |
108,9 |
96,5 |
a |
| TB client 5 years and older start on treatment rate |
2019/20 |
DHIS |
97,0 |
98,3 |
97,6 |
95,5 |
99,0 |
98,8 |
101,1 |
99,5 |
99,9 |
90,0 |
a |
| 2020/21 |
DHIS |
94,8 |
93,0 |
93,2 |
93,4 |
96,4 |
96,2 |
96,0 |
99,8 |
95,3 |
90,3 |
a |
| 2021/22 |
DHIS |
93,4 |
92,7 |
90,6 |
94,8 |
94,8 |
97,2 |
93,4 |
87,9 |
95,3 |
91,4 |
a |
| TB DS client lost to follow up rate |
2019 |
both sexes DHIS |
12,6 |
13,8 |
10,8 |
8,5 |
10,0 |
9,6 |
10,5 |
18,8 |
12,4 |
18,6 |
a |
| 2020 |
both sexes DHIS |
12,0 |
13,3 |
11,6 |
7,9 |
8,4 |
7,7 |
8,4 |
22,1 |
10,0 |
18,8 |
a |
| 2021 |
both sexes DHIS |
13,0 |
14,5 |
14,3 |
7,5 |
9,1 |
7,1 |
7,0 |
25,2 |
7,8 |
20,7 |
a |
| TB DS death rate |
2019 |
both sexes DHIS |
7,4 |
7,5 |
10,6 |
7,4 |
7,5 |
12,5 |
9,0 |
7,3 |
9,5 |
3,9 |
a |
| 2020 |
both sexes DHIS |
8,3 |
7,7 |
12,5 |
9,2 |
8,0 |
13,7 |
10,4 |
8,4 |
10,3 |
5,2 |
a |
| 2021 |
both sexes DHIS |
8,3 |
8,0 |
13,4 |
9,5 |
8,1 |
13,3 |
9,6 |
8,6 |
9,1 |
5,2 |
a |
| TB DS treatment success rate |
2019 |
both sexes DHIS |
79,3 |
77,9 |
77,3 |
83,6 |
81,9 |
77,2 |
80,0 |
72,6 |
77,6 |
76,5 |
a |
| 2020 |
both sexes DHIS |
78,9 |
78,2 |
74,6 |
82,4 |
83,0 |
77,7 |
80,6 |
68,4 |
79,1 |
74,9 |
a |
| 2021 |
both sexes DHIS |
77,9 |
76,6 |
71,3 |
82,5 |
82,1 |
78,9 |
82,8 |
64,9 |
82,1 |
73,0 |
a |
| TB MDR client death rate |
2019 |
both sexes DHIS |
16,6 |
18,6 |
26,7 |
18,4 |
13,4 |
24,3 |
20,9 |
13,7 |
16,8 |
13,3 |
a |
| 2020 |
both sexes DHIS |
17,5 |
19,2 |
26,6 |
19,1 |
16,0 |
17,8 |
20,0 |
20,1 |
16,6 |
13,6 |
a |
| TB MDR client loss to follow up rate |
2019 |
both sexes DHIS |
15,2 |
16,5 |
10,7 |
15,3 |
13,2 |
8,1 |
6,6 |
21,5 |
10,7 |
22,8 |
a |
| 2020 |
both sexes DHIS |
16,5 |
16,8 |
11,2 |
16,9 |
13,9 |
11,7 |
9,4 |
16,0 |
9,4 |
25,5 |
a |
| TB MDR treatment success rate |
2019 |
both sexes EDRWeb |
60,7 |
60,4 |
59,1 |
58,7 |
66,0 |
55,8 |
66,3 |
60,3 |
65,4 |
51,6 |
a |
| 2020 |
both sexes DHIS |
60,8 |
60,1 |
56,1 |
60,5 |
66,1 |
64,3 |
68,5 |
61,2 |
65,8 |
51,3 |
a |
| TB symptom 5 years and older screened in facility rate |
2019/20 |
both sexes DHIS |
88,6 |
85,7 |
110,1 |
98,1 |
99,7 |
95,3 |
87,1 |
68,9 |
76,6 |
53,4 |
a |
| 2020/21 |
both sexes DHIS |
87,6 |
85,7 |
85,9 |
98,9 |
98,3 |
88,9 |
86,1 |
65,2 |
70,9 |
61,9 |
a |
| 2021/22 |
both sexes DHIS |
95,8 |
90,6 |
89,3 |
111,4 |
104,9 |
95,2 |
95,7 |
80,1 |
80,0 |
72,5 |
a |
| TB symptom child under 5 years screened in facility rate |
2019/20 |
both sexes DHIS |
87,6 |
85,4 |
109,5 |
87,3 |
98,2 |
88,0 |
90,5 |
64,8 |
70,3 |
71,5 |
a |
| 2020/21 |
both sexes DHIS |
88,9 |
91,8 |
95,8 |
90,7 |
101,4 |
83,9 |
94,7 |
69,1 |
65,4 |
73,9 |
a |
| 2021/22 |
both sexes DHIS |
92,6 |
95,5 |
97,7 |
95,8 |
100,9 |
88,2 |
96,1 |
83,3 |
74,3 |
80,6 |
a |
| TB XDR client death rate |
2019 |
both sexes DHIS |
19,1 |
19,7 |
35,7 |
27,6 |
10,4 |
50,0 |
31,3 |
14,3 |
0,0 |
17,7 |
a |
| 2020 |
both sexes DHIS |
16,5 |
19,2 |
0,0 |
17,4 |
13,7 |
0,0 |
16,7 |
21,4 |
|
5,9 |
a |
| TB XDR client loss to follow up rate |
2019 |
both sexes DHIS |
12,1 |
10,9 |
7,1 |
6,9 |
11,7 |
0,0 |
12,5 |
28,6 |
0,0 |
16,1 |
a |
| 2020 |
both sexes DHIS |
17,8 |
19,2 |
25,0 |
8,7 |
15,7 |
0,0 |
33,3 |
28,6 |
|
11,8 |
a |
| TB XDR started on treatment |
2019 |
both sexes DHIS |
461 |
239 |
14 |
29 |
77 |
2 |
16 |
21 |
1 |
62 |
a |
| 2020 |
both sexes DHIS |
315 |
182 |
4 |
23 |
51 |
1 |
6 |
14 |
0 |
34 |
a |
| TB XDR successfully complete treatment |
2019 |
both sexes DHIS |
284 |
152 |
7 |
18 |
58 |
1 |
7 |
10 |
1 |
30 |
a |
| 2020 |
both sexes DHIS |
169 |
94 |
0 |
14 |
28 |
0 |
3 |
6 |
0 |
24 |
a |
| TB XDR treatment success rate |
2019 |
both sexes EDRWeb |
49,9 |
52,1 |
46,2 |
51,7 |
55,8 |
50,0 |
25,0 |
47,6 |
0,0 |
41,9 |
a |
| 2020 |
both sexes DHIS |
53,7 |
51,6 |
0,0 |
60,9 |
54,9 |
0,0 |
50,0 |
42,9 |
|
70,6 |
a |
Reference notes
a webDHIS.10
b Global TB Report 2022.54
c World Health Statistics 2021.31
d World Health Statistics 2022.32
Definitions
- All DS TB patients in cohort [Number].
- DS TB patients who completed treatment or were cured [Number].
- Screen for TB symptoms 5 years and older [Number]: Clients 5 years and older who were screened in health facilities for TB symptoms using the standard TB screening tool as per National TB Guideline.
- Screen for TB symptoms under 5 years [Number]: Children under 5 years who were screened in health facilities for TB symptoms using the standard TB screening tool as per National TB Guideline.
- TB XDR started on treatment [Number]: Number of XDR-TB patients who started treatment.
- TB XDR successfully complete treatment [Number]: Extensive Drug Resistant TB (XDR-TB) clients successfully treated at the end of the treatment.
- TB child under 5 years start on treatment rate [Percentage]: TB client under 5 years started on treatment as a proportion of ALL symptomatic children under 5 years.
- TB client 5 years and older start on treatment rate [Percentage]: TB client 5 years and older start on treatment as a proportion of TB symptomatic client 5 years and older test positive.
- TB DS client lost to follow-up rate [Percentage]: The percentage of TB clients (all types of TB) who defaulted treatment.
- TB DS death rate [Percentage]: The percentage of TB clients (all types of TB registered in ETR.net) who died.
- TB DS treatment success rate [Percentage]: The percentage of TB clients (all types registered in ETR.net) cured plus those who completed treatment.
- TB MDR client death rate [Percentage]: The percentage of TB clients (MDR TB) who died.
- TB MDR client loss to follow-up rate [Percentage]: The percentage of TB clients (MDR TB) who are lost to follow-up.
- TB MDR treatment success rate [Percentage]: The percentage of TB clients (MDR TB) cured plus those who completed treatment.
- TB symptom child under 5 years screened in facility rate [Percentage]: Children under 5 years screened for TB symptoms as a proportion of PHC headcount under 5 years.
- TB XDR client death rate [Percentage]: The percentage of TB clients (XDR TB) who died.
- TB XDR client loss to follow-up rate [Percentage]: The percentage of TB clients (XDR TB) who are lost to follow-up.
- TB XDR treatment success rate [Percentage]: TB XDR clients successfully complete treatment as a proportion of TB XDR clients started on treatment.
Figure 11 shows that preventive therapy for children under 5 years (shown in light blue) declined in performance consistently over the 2019-2022 period. This is particularly concerning as TB is very difficult to diagnose in children under 5 years, as the children are unable to articulate their symptoms, and parents find it challenging, or are sometimes unaware of, the changes to take note of in their children that would indicate the presence of TB. As such, TB in children under 5 years of age must become an explicit area of focus for TB programmes in South Africa. Gastric washout is the most commonly used procedure to diagnose TB in children under 5 years of age; however, it is a very invasive procedure that makes parents reluctant to provide consent, among other factors. A few clinical research initiatives have attempted to solve this challenge. However, data indicate that these types of research initiatives need to be prioritised and invested in so that there can be accelerated learning and calibration, and treatment can be rolled out as soon as possible to this high-TB-risk population subset.

Figure 11.National TB performance against targets, 2018-2022
5.4. HIV and AIDS
Figure 12 shows that by March 2022, the number of HIV tests performed nationally appeared to have recovered to pre-pandemic levels. However, the impact of the COVID-19 pandemic on HIV response should not be under-estimated as the figures for March 2022 were lower than what was forecasted. Figure 13 shows the same trend for most provinces with the exception of the Northern and Western Cape and Limpopo where HIV testing numbers had reached the estimated forecasted levels for March 2022. Figure 14 to Figure 16 graphically illustrate the impact on treatment initiations and retention in care. In a high HIV and TB burden setting, COVID-19 has been associated with high mortality among people living with HIV.60 A divergence is noted in the antiretroviral effective coverage figures between the modelled Thembisa 4.5 estimates and the routine coverage from webDHIS (Table 13), which could be the result of the momentum lost during the COVID-19 period.
__january_2020_-_march_2022.png)
Figure 12.HIV tests done (national), January 2020 - March 2022
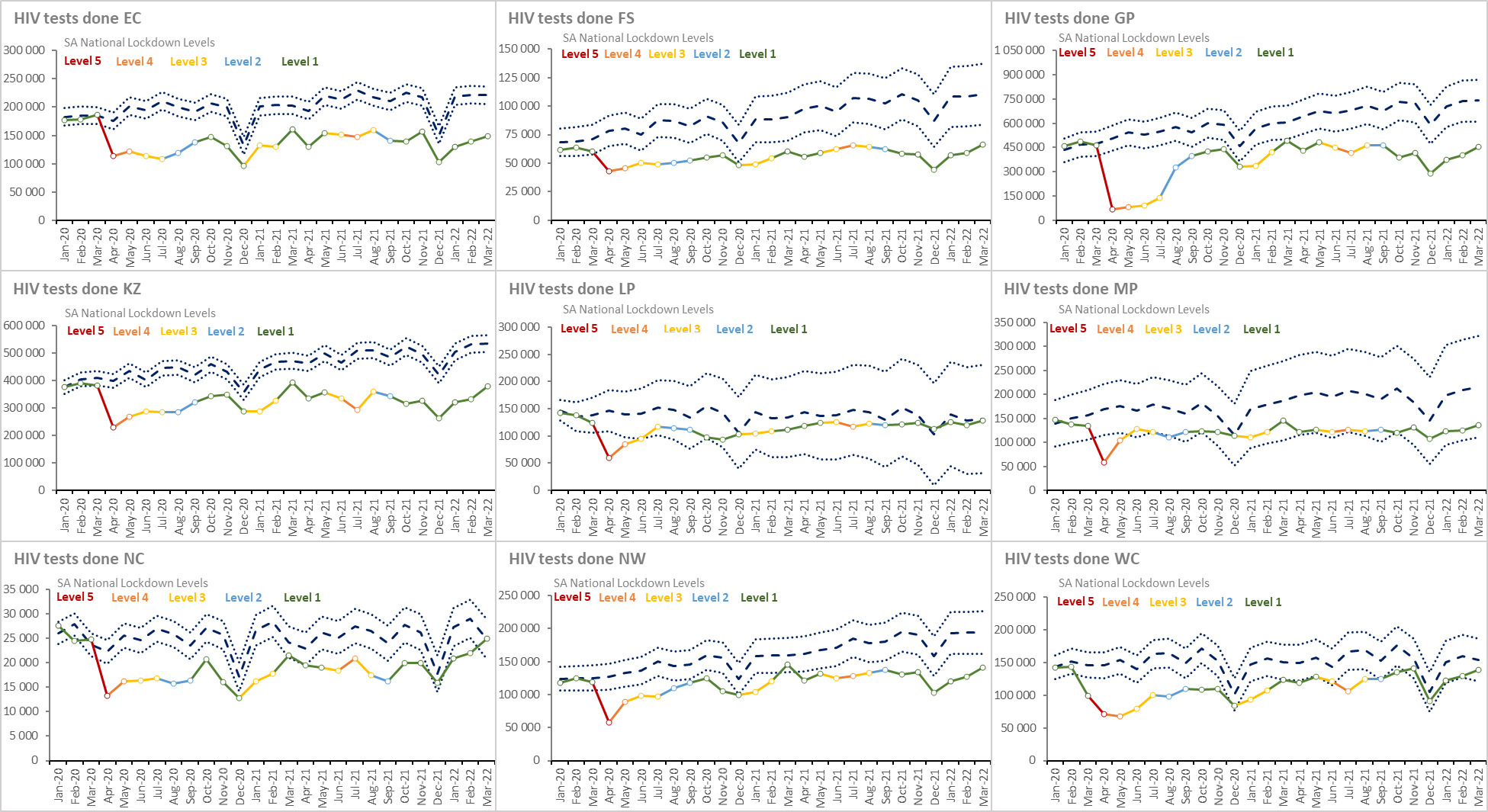
Figure 13.HIV tests per province, January 2020 - March 2022
__january_2020_-_march_2022.png)
Figure 14.ART client start ART during month (national), January 2020 - March 2022

Figure 15.ART client start ART during month by province, January 2020 - March 2022
__january_2020_-_march_2022.png)
Figure 16.ART client remain on ART (national), January 2020 - March 2022
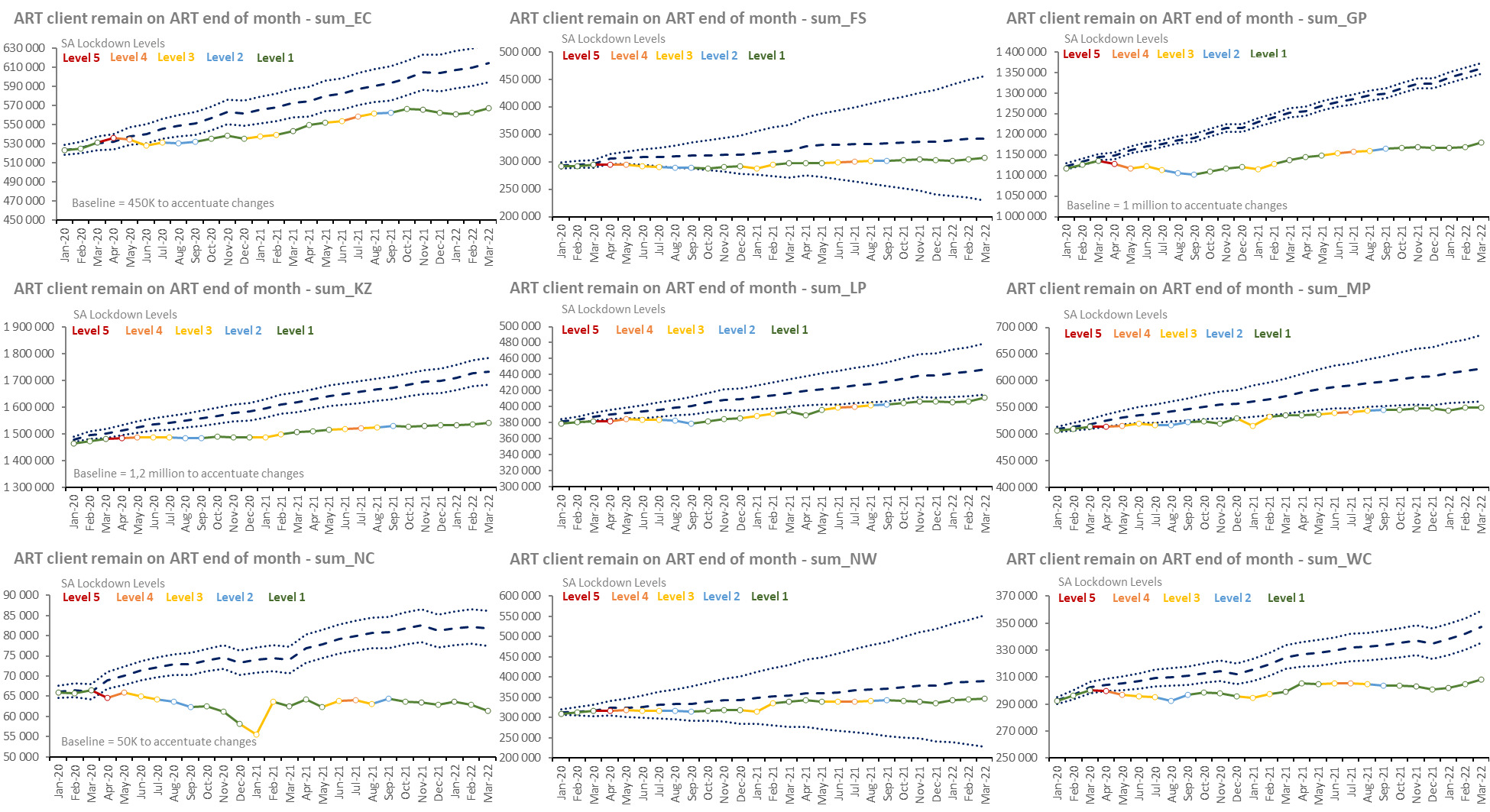
Figure 17.ART client remain on ART by province, January 2020 - March 2022
Table 13.HIV and AIDS indicators by province, 2018- 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Adult living with HIV |
2020 Q1 |
both sexes 15+ years NDoH-Thembisa |
7 174 336 |
808 940 |
403 021 |
1 866 419 |
1 950 240 |
461 625 |
668 118 |
79 737 |
501 315 |
434 921 |
a |
| 2021 Q1 |
both sexes 15+ years NDoH-Thembisa |
7 157 513 |
820 796 |
396 195 |
1 752 754 |
1 854 967 |
567 873 |
683 117 |
101 051 |
498 164 |
482 596 |
a |
| 2022 Q1 |
both sexes 15+ years NDoH-Thembisa |
7 518 945 |
833 869 |
389 880 |
1 836 580 |
1 911 616 |
664 333 |
717 174 |
103 808 |
514 813 |
546 872 |
a |
| Child living with HIV |
2020 Q1 |
both sexes 0-14 years NDoH-Thembisa |
326 567 |
42 576 |
19 529 |
58 700 |
100 371 |
27 699 |
35 720 |
4 862 |
23 536 |
13 574 |
a |
| 2021 Q1 |
both sexes 0-14 years NDoH-Thembisa |
268 935 |
36 519 |
17 079 |
48 685 |
73 354 |
27 081 |
26 420 |
5 854 |
18 756 |
15 187 |
a |
| 2022 Q1 |
both sexes 0-14 years NDoH-Thembisa |
270 599 |
32 056 |
14 767 |
49 277 |
75 076 |
30 986 |
31 336 |
4 428 |
18 645 |
14 028 |
a |
| Total living with HIV |
2020 Q1 |
both sexes all ages NDoH-Thembisa |
7 500 903 |
851 516 |
422 550 |
1 925 119 |
2 050 611 |
489 324 |
703 838 |
84 599 |
524 851 |
448 495 |
a |
| 2021 Q1 |
both sexes all ages NDoH-Thembisa |
7 426 448 |
857 315 |
413 274 |
1 801 439 |
1 928 321 |
594 954 |
709 537 |
106 905 |
516 920 |
497 783 |
a |
| 2022 Q1 |
both sexes all ages NDoH-Thembisa |
7 789 544 |
865 925 |
404 647 |
1 885 857 |
1 986 692 |
695 319 |
748 510 |
108 236 |
533 458 |
560 900 |
a |
| People living with HIV (PLHIV) |
2020 |
both sexes 0-14 years Global Report |
310 000 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages Global Report |
7 800 000 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages mid-year |
7 800 000 |
|
|
|
|
|
|
|
|
|
c |
| both sexes all ages Thembisa 4.4 |
7 892 070 |
863 517 |
404 619 |
1 878 400 |
1 985 710 |
692 685 |
746 915 |
107 814 |
532 097 |
556 517 |
d |
| both sexes ILO in labour force |
4 887 632 |
|
|
|
|
|
|
|
|
|
e |
| female 15 + years Global Report |
4 800 000 |
|
|
|
|
|
|
|
|
|
b |
| female ILO in labour force |
2 607 391 |
|
|
|
|
|
|
|
|
|
e |
| male 15+ years Global Report |
2 700 000 |
|
|
|
|
|
|
|
|
|
b |
| male ILO in labour force |
2 280 241 |
|
|
|
|
|
|
|
|
|
e |
| 2021 |
both sexes all ages Thembisa 4.4 |
8 008 080 |
874 329 |
405 266 |
1 910 980 |
1 992 300 |
704 108 |
754 254 |
109 608 |
538 115 |
574 861 |
d |
| 2022 |
both sexes all ages Thembisa 4.5 |
7 975 940 |
900 332 |
415 029 |
1 849 650 |
2 034 810 |
706 564 |
752 696 |
112 561 |
544 074 |
586 425 |
f |
Percentage of people living with HIV (PLHIV)
who know their status (1st 90) |
2019 |
both sexes all ages Global Report |
92,0 |
|
|
|
|
|
|
|
|
|
g |
| female 15+ years Global Report |
94,0 |
|
|
|
|
|
|
|
|
|
g |
| male 15+ years Global Report |
91,0 |
|
|
|
|
|
|
|
|
|
g |
| 2020 |
both sexes 0-14 years Global Report |
75,0 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages Global Report |
92,0 |
|
|
|
|
|
|
|
|
|
b |
| female 15+ years Global Report |
94,0 |
|
|
|
|
|
|
|
|
|
b |
| male 15 years Global Report |
91,0 |
|
|
|
|
|
|
|
|
|
b |
| HIV prevalence (age 15-49) |
2020 |
both sexes 15-49 years mid-year |
18,7 |
|
|
|
|
|
|
|
|
|
c |
| female 15-49 years mid-year |
23,0 |
|
|
|
|
|
|
|
|
|
c |
| 2021 |
both sexes mid-year |
19,5 |
|
|
|
|
|
|
|
|
|
h |
| 2022 |
both sexes mid-year |
19,6 |
|
|
|
|
|
|
|
|
|
i |
| HIV prevalence (total population) |
2020 |
both sexes all ages mid-year |
13,0 |
|
|
|
|
|
|
|
|
|
c |
| both sexes all ages Thembisa 4.3 |
13,2 |
13,7 |
15,0 |
12,4 |
17,9 |
10,8 |
15,9 |
9,9 |
13,8 |
7,6 |
j |
| both sexes all ages Thembisa 4.4 |
13,4 |
13,3 |
14,0 |
12,0 |
17,6 |
11,9 |
15,6 |
9,6 |
13,3 |
8,1 |
d |
| both sexes ILO in labour force |
23,9 |
|
|
|
|
|
|
|
|
|
e |
| female ILO in labour force |
30,2 |
|
|
|
|
|
|
|
|
|
e |
| male ILO in labour force |
19,3 |
|
|
|
|
|
|
|
|
|
e |
| 2021 |
both sexes all ages Thembisa 4.4 |
13,4 |
13,4 |
14,0 |
12,0 |
17,5 |
12,0 |
15,5 |
9,7 |
13,2 |
8,2 |
d |
| both sexes mid-year |
13,7 |
|
|
|
|
|
|
|
|
|
h |
| 2022 |
both sexes all ages Thembisa 4.5 |
13,5 |
14,1 |
14,7 |
11,8 |
18,1 |
12,0 |
15,8 |
10,1 |
13,6 |
8,4 |
f |
| both sexes mid-year |
13,9 |
|
|
|
|
|
|
|
|
|
i |
| Adult ART Total |
2020 Q1 |
both sexes 15+ years DHIS |
4 866 047 |
511 867 |
282 727 |
1 109 761 |
1 436 613 |
366 875 |
498 211 |
61 567 |
305 498 |
292 928 |
a |
| 2021 Q1 |
both sexes 15+ years DHIS |
4 981 934 |
526 288 |
288 816 |
1 115 574 |
1 467 110 |
381 963 |
520 366 |
58 798 |
331 156 |
291 863 |
a |
| 2022 Q1 |
both sexes 15+ years DHIS |
5 148 692 |
551 615 |
298 996 |
1 160 906 |
1 506 479 |
399 243 |
534 821 |
57 815 |
338 111 |
300 706 |
a |
| Child ART Total |
2020 Q1 |
both sexes 0-14 years DHIS |
148 396 |
18 849 |
10 151 |
23 425 |
44 482 |
13 755 |
16 394 |
4 015 |
9 295 |
8 030 |
a |
| 2021 Q1 |
both sexes 0-14 years DHIS |
135 459 |
17 284 |
8 204 |
21 088 |
41 226 |
12 372 |
15 602 |
3 673 |
8 516 |
7 494 |
a |
| 2022 Q1 |
both sexes 0-14 years DHIS |
123 135 |
16 224 |
7 401 |
19 191 |
35 473 |
11 638 |
14 726 |
3 511 |
7 669 |
7 302 |
a |
| Number of patients receiving ART |
2020 |
both sexes all ages Thembisa 4.3 |
5 286 810 |
559 312 |
297 082 |
1 181 960 |
1 465 490 |
404 000 |
493 116 |
72 224 |
315 454 |
334 966 |
j |
| both sexes all ages Thembisa 4.4 |
4 976 670 |
565 489 |
299 766 |
1 175 690 |
1 522 030 |
405 754 |
539 588 |
69 361 |
334 696 |
315 474 |
d |
| 2020 Q1 |
both sexes all ages DHIS |
5 014 443 |
530 716 |
292 878 |
1 133 186 |
1 481 095 |
380 630 |
514 605 |
65 582 |
314 793 |
300 958 |
a |
| 2021 |
both sexes all ages Thembisa 4.4 |
5 240 800 |
590 495 |
306 668 |
1 219 410 |
1 557 130 |
426 306 |
562 597 |
72 965 |
349 713 |
334 444 |
d |
| 2021 Q1 |
both sexes all ages DHIS |
5 111 503 |
542 488 |
295 260 |
1 136 123 |
1 508 568 |
394 362 |
533 347 |
62 383 |
339 532 |
299 440 |
a |
| 2022 |
both sexes all ages Thembisa 4.5 |
5 631 460 |
592 901 |
315 868 |
1 249 670 |
1 583 250 |
437 523 |
562 923 |
70 949 |
359 946 |
336 590 |
f |
| 2022 Q1 |
both sexes all ages DHIS |
5 271 827 |
567 839 |
306 397 |
1 180 097 |
1 541 952 |
410 881 |
549 547 |
61 326 |
345 780 |
308 008 |
a |
| Total Clients remaining on ART at the end of the month |
Mar 2020 |
both sexes all ages DHIS |
5 020 308 |
531 135 |
294 215 |
1 134 719 |
1 481 679 |
381 733 |
514 347 |
66 439 |
315 571 |
300 470 |
a |
| Mar 2021 |
both sexes all ages DHIS |
5 117 541 |
543 572 |
296 971 |
1 136 662 |
1 508 336 |
394 335 |
536 165 |
62 471 |
339 672 |
299 357 |
a |
| Mar 2022 |
both sexes 15+ years DHIS |
5 271 827 |
567 839 |
306 397 |
1 180 097 |
1 541 952 |
410 881 |
549 547 |
61 326 |
345 780 |
308 008 |
a |
| Antiretroviral coverage (2nd 90) |
2020 |
both sexes 0-14 years Global Report |
47,0 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages GBD |
72,8 |
|
|
|
|
|
|
|
|
|
k |
| both sexes all ages Global Report |
72,0 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages Thembisa 4.3 |
68,4 |
61,7 |
67,4 |
61,8 |
71,4 |
64,5 |
65,3 |
64,0 |
57,7 |
64,4 |
j |
| both sexes all ages Thembisa 4.4 |
71,9 |
71,4 |
80,2 |
68,1 |
81,3 |
64,8 |
78,3 |
70,5 |
68,7 |
62,3 |
d |
| female 15+ years Global Report |
78,0 |
|
|
|
|
|
|
|
|
|
b |
| male 15 years Global Report |
63,0 |
|
|
|
|
|
|
|
|
|
b |
| 2021 |
both sexes all ages Thembisa 4.4 |
73,7 |
73,3 |
81,5 |
69,6 |
82,5 |
66,6 |
80,4 |
72,8 |
70,7 |
64,0 |
d |
| 2022 |
both sexes all ages Thembisa 4.5 |
75,0 |
71,3 |
80,9 |
72,2 |
81,1 |
67,9 |
79,2 |
69,1 |
70,9 |
62,4 |
f |
| Clients remaining on ART rate |
Mar 2020 |
both sexes all ages DHIS |
66,9 |
62,4 |
69,4 |
58,9 |
72,2 |
77,8 |
73,1 |
77,5 |
59,9 |
67,1 |
a |
| Mar 2021 |
both sexes all ages DHIS |
68,9 |
63,4 |
71,9 |
63,1 |
78,2 |
66,3 |
75,6 |
58,4 |
65,7 |
60,1 |
a |
| Mar 2022 |
both sexes all ages DHIS |
67,7 |
65,6 |
75,7 |
62,6 |
77,6 |
59,1 |
73,4 |
56,7 |
64,8 |
54,9 |
a |
| Antiretroviral effective coverage |
2020 |
both sexes all ages Thembisa 4.3 |
63,3 |
56,0 |
63,5 |
55,3 |
67,6 |
57,6 |
60,2 |
58,4 |
52,9 |
60,6 |
j |
| both sexes all ages Thembisa 4.4 |
66,4 |
65,5 |
74,1 |
62,6 |
76,7 |
58,6 |
72,2 |
64,4 |
62,9 |
56,7 |
d |
| 2020 Q1 |
both sexes 0-14 years DHIS-Tier |
18,7 |
19,1 |
17,4 |
18,8 |
21,2 |
19,1 |
20,2 |
13,9 |
17,5 |
|
a |
| both sexes 15+ years DHIS-Tier |
41,8 |
37,8 |
39,9 |
41,6 |
49,0 |
53,6 |
52,5 |
17,8 |
37,7 |
|
a |
| both sexes all ages DHIS-Tier |
40,8 |
36,8 |
38,8 |
40,9 |
47,6 |
51,6 |
50,8 |
17,6 |
36,8 |
|
a |
| 2021 |
both sexes all ages Thembisa 4.4 |
68,3 |
67,6 |
75,7 |
63,8 |
78,2 |
60,6 |
74,6 |
66,6 |
65,0 |
58,2 |
d |
| 2021 Q1 |
both sexes all ages DHIS-Tier |
45,5 |
39,9 |
43,9 |
45,0 |
52,6 |
44,2 |
50,3 |
22,5 |
43,5 |
32,6 |
a |
| 2022 |
both sexes all ages Thembisa 4.5 |
70,6 |
65,9 |
76,1 |
67,6 |
77,8 |
61,9 |
74,8 |
63,1 |
66,2 |
57,4 |
f |
| 2022 Q1 |
both sexes all ages DHIS-Tier |
45,1 |
40,0 |
49,9 |
45,3 |
56,0 |
36,5 |
50,6 |
21,5 |
43,8 |
20,0 |
a |
| Adult with viral load suppressed rate 12 months |
2020 Q1 |
both sexes 15+ years DHIS |
88,1 |
86,8 |
89,7 |
87,6 |
90,6 |
86,5 |
86,2 |
83,6 |
85,5 |
|
a |
| 2021 Q1 |
both sexes 15+ years DHIS |
88,6 |
88,6 |
89,3 |
88,7 |
89,1 |
88,3 |
88,3 |
83,3 |
86,5 |
90,3 |
a |
| 2022 Q1 |
both sexes 15+ years DHIS |
88,9 |
86,7 |
92,8 |
91,3 |
90,5 |
79,9 |
87,7 |
85,0 |
84,3 |
91,6 |
a |
| Child with viral load suppressed rate 12 months |
2020 Q1 |
both sexes 0-14 years DHIS |
63,9 |
62,9 |
64,3 |
64,3 |
68,8 |
51,5 |
60,9 |
75,2 |
65,3 |
|
a |
| 2021 Q1 |
both sexes 0-14 years DHIS |
65,3 |
62,3 |
72,5 |
65,2 |
53,1 |
68,4 |
64,0 |
69,8 |
68,0 |
64,5 |
a |
| 2022 Q1 |
both sexes 0-14 years DHIS |
60,7 |
63,2 |
61,4 |
63,2 |
55,8 |
62,3 |
53,1 |
|
59,4 |
69,3 |
a |
| ART client viral load suppressed rate (VLS) |
2020 Q1 |
both sexes all ages DHIS-Tier |
87,5 |
85,9 |
89,0 |
87,1 |
89,9 |
85,3 |
85,5 |
83,2 |
84,9 |
|
a |
| 2021 Q1 |
both sexes all ages DHIS |
88,0 |
87,8 |
89,1 |
88,3 |
88,5 |
87,3 |
87,7 |
81,5 |
86,1 |
88,6 |
a |
| 2022 Q1 |
both sexes all ages DHIS |
88,0 |
86,0 |
92,0 |
91,0 |
90,0 |
79,0 |
87,0 |
84,0 |
84,0 |
91,0 |
a |
| HIV viral load suppression (3rd 90) |
2020 |
both sexes 0-14 years Global Report |
33,0 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages Global Report |
66,0 |
|
|
|
|
|
|
|
|
|
b |
| both sexes all ages Thembisa 4.3 |
92,5 |
90,6 |
94,1 |
89,4 |
94,6 |
89,3 |
92,3 |
91,2 |
91,7 |
94,2 |
j |
| both sexes all ages Thembisa 4.4 |
59,6 |
57,1 |
68,8 |
55,4 |
71,0 |
51,0 |
64,3 |
57,7 |
56,2 |
52,7 |
d |
| female 15+ years Global Report |
72,0 |
|
|
|
|
|
|
|
|
|
b |
| male 15 years Global Report |
58,0 |
|
|
|
|
|
|
|
|
|
b |
| 2021 |
both sexes all ages Thembisa 4.4 |
62,8 |
60,8 |
71,5 |
58,2 |
73,7 |
54,4 |
68,2 |
61,2 |
59,7 |
55,1 |
d |
| 2022 |
both sexes all ages Thembisa 4.5 |
64,0 |
57,4 |
70,6 |
60,7 |
72,2 |
53,9 |
67,6 |
55,8 |
60,0 |
53,6 |
f |
| Infant PCR test positive around 10 weeks rate |
2018/19 |
both sexes DHIS |
0,7 |
1,0 |
0,7 |
0,7 |
0,6 |
0,7 |
0,9 |
1,4 |
0,9 |
0,3 |
a |
| 2019/20 |
both sexes DHIS |
0,7 |
0,9 |
0,5 |
0,7 |
0,5 |
0,7 |
0,9 |
1,3 |
0,9 |
0,3 |
a |
| 2020/21 |
both sexes DHIS |
0,6 |
0,7 |
0,5 |
0,7 |
0,4 |
0,7 |
0,6 |
1,0 |
0,7 |
0,3 |
a |
| Adult living with HIV viral load done 12m |
2020 Q1 |
both sexes 15+ years DHIS-Tier |
3 403 846 |
352 021 |
179 121 |
886 716 |
1 055 123 |
286 134 |
406 715 |
16 964 |
221 052 |
|
a |
| 2021 Q1 |
both sexes 15+ years DHIS |
3 734 509 |
377 554 |
198 456 |
898 715 |
1 111 108 |
292 891 |
396 112 |
27 698 |
255 405 |
176 570 |
a |
| 2022 Q1 |
both sexes 15+ years DHIS |
3 899 389 |
391 707 |
214 659 |
924 923 |
1 210 061 |
312 055 |
425 359 |
27 427 |
273 492 |
119 706 |
a |
| Adult living with HIV viral load suppressed (VLS) 12m |
2020 Q1 |
both sexes 15+ years DHIS |
2 999 406 |
305 530 |
160 656 |
776 624 |
955 434 |
247 396 |
350 673 |
14 188 |
188 905 |
|
a |
| 2021 Q1 |
both sexes 15+ years DHIS |
3 317 696 |
334 432 |
178 051 |
799 532 |
992 743 |
258 942 |
350 454 |
23 238 |
220 859 |
159 445 |
a |
| 2022 Q1 |
both sexes 15+ years DHIS |
3 464 855 |
339 499 |
199 254 |
844 446 |
1 095 505 |
249 401 |
373 072 |
23 306 |
230 668 |
109 704 |
a |
| Adult remaining on ART at end of the month - total |
Mar 2020 |
both sexes 15+ years DHIS |
4 872 515 |
512 268 |
284 952 |
1 111 128 |
1 437 205 |
367 756 |
497 964 |
62 524 |
306 262 |
292 456 |
a |
| Mar 2021 |
both sexes 15+ years DHIS |
4 980 854 |
526 288 |
288 767 |
1 115 574 |
1 467 110 |
381 963 |
519 335 |
58 798 |
331 156 |
291 863 |
a |
| Mar 2022 |
both sexes 15+ years DHIS |
5 148 692 |
551 615 |
298 996 |
1 160 906 |
1 506 479 |
399 243 |
534 821 |
57 815 |
338 111 |
300 706 |
a |
| Antenatal client initiated on ART rate |
2019/20 |
female DHIS |
96,2 |
95,3 |
98,4 |
97,2 |
98,4 |
95,2 |
98,8 |
93,4 |
98,1 |
80,2 |
a |
| 2020/21 |
female DHIS |
94,9 |
91,8 |
98,1 |
98,6 |
98,9 |
96,8 |
96,6 |
88,6 |
93,2 |
67,9 |
a |
| 2021/22 |
female DHIS |
95,0 |
90,4 |
97,7 |
99,3 |
98,9 |
98,0 |
97,6 |
90,4 |
90,3 |
68,5 |
a |
| Antenatal client start on ART |
2019/20 |
female DHIS |
94 440 |
10 536 |
4 126 |
25 746 |
21 207 |
9 871 |
10 526 |
1 563 |
6 020 |
4 845 |
a |
| 2020/21 |
female DHIS |
82 021 |
8 893 |
3 451 |
22 662 |
18 524 |
8 853 |
9 450 |
1 389 |
4 993 |
3 806 |
a |
| 2021/22 |
female DHIS |
68 045 |
7 827 |
3 173 |
17 969 |
16 121 |
7 358 |
7 041 |
1 210 |
4 090 |
3 256 |
a |
| Child living with HIV viral load done 12m |
2020 Q1 |
both sexes 0-14 years DHIS-Tier |
95 581 |
12 927 |
5 290 |
17 137 |
30 907 |
10 262 |
11 865 |
898 |
6 295 |
|
a |
| 2021 Q1 |
both sexes 0-14 years DHIS |
93 422 |
11 737 |
4 852 |
16 731 |
31 182 |
7 988 |
9 986 |
1 186 |
5 526 |
4 234 |
a |
| 2022 Q1 |
both sexes 0-14 years DHIS |
84 890 |
10 748 |
4 293 |
14 590 |
27 318 |
8 134 |
10 702 |
180 |
5 445 |
3 480 |
a |
| Child living with HIV viral load suppressed (VLS) 12m |
2020 Q1 |
both sexes 0-14 years DHIS |
61 099 |
8 127 |
3 400 |
11 021 |
21 255 |
5 284 |
7 227 |
675 |
4 110 |
|
a |
| 2021 Q1 |
both sexes 0-14 years DHIS |
61 022 |
7 309 |
3 520 |
10 916 |
21 329 |
4 243 |
6 387 |
828 |
3 760 |
2 730 |
a |
| 2022 Q1 |
both sexes 0-14 years DHIS |
51 530 |
6 790 |
2 634 |
9 224 |
17 022 |
4 535 |
5 679 |
|
3 235 |
2 411 |
a |
| Child under 15 years remaining on ART at end of the month - total |
2021 Q1 |
both sexes 0-14 years DHIS |
136 687 |
17 284 |
8 204 |
21 088 |
41 226 |
12 372 |
16 830 |
3 673 |
8 516 |
7 494 |
a |
| Mar 2020 |
both sexes 0-14 years DHIS |
147 793 |
18 867 |
9 263 |
23 591 |
44 474 |
13 977 |
16 383 |
3 915 |
9 309 |
8 014 |
a |
| Mar 2022 |
both sexes 0-14 years DHIS |
123 135 |
16 224 |
7 401 |
19 191 |
35 473 |
11 638 |
14 726 |
3 511 |
7 669 |
7 302 |
a |
| HIV testing coverage |
2020 |
both sexes 15+ years Thembisa 4.3 |
77,7 |
74,0 |
73,1 |
75,9 |
79,0 |
75,1 |
74,6 |
75,1 |
76,7 |
76,2 |
j |
| both sexes 15+ years Thembisa 4.4 |
77,7 |
75,7 |
75,4 |
79,0 |
80,9 |
76,4 |
77,0 |
76,5 |
79,2 |
78,1 |
d |
| 2021 |
both sexes 15+ years Thembisa 4.4 |
78,2 |
76,5 |
75,8 |
79,2 |
81,7 |
77,1 |
77,6 |
77,0 |
79,7 |
78,6 |
d |
| 2022 |
both sexes 15+ years Thembisa 4.5 |
82,9 |
79,9 |
75,5 |
83,8 |
86,2 |
78,4 |
77,8 |
77,7 |
82,5 |
82,4 |
f |
| Infant 1st PCR test positive at birth rate |
2019/20 |
both sexes DHIS |
0,6 |
0,5 |
0,4 |
0,5 |
0,3 |
0,6 |
1,0 |
0,4 |
1,3 |
0,8 |
a |
| 2020/21 |
both sexes DHIS |
0,5 |
0,5 |
0,3 |
0,6 |
0,4 |
0,5 |
0,8 |
0,6 |
0,6 |
0,8 |
a |
| 2021/22 |
both sexes DHIS |
0,4 |
0,4 |
0,1 |
0,5 |
0,3 |
0,5 |
0,3 |
0,8 |
0,5 |
0,8 |
a |
| Medical male circumcision 15 years and older rate |
2019/20 |
DHIS |
46,4 |
59,5 |
32,2 |
38,3 |
47,6 |
24,4 |
52,5 |
51,6 |
61,1 |
71,2 |
a |
| 2020/21 |
DHIS |
59,1 |
88,6 |
73,5 |
38,9 |
79,2 |
85,9 |
67,4 |
59,8 |
94,5 |
91,2 |
a |
| 2021/22 |
DHIS |
55,8 |
79,3 |
50,3 |
38,5 |
60,1 |
78,7 |
68,6 |
40,5 |
84,3 |
92,5 |
a |
| Percentage of deaths due to AIDS |
2020 |
both sexes all ages mid-year |
15,4 |
|
|
|
|
|
|
|
|
|
c |
| 2021 |
both sexes all ages mid-year |
12,2 |
|
|
|
|
|
|
|
|
|
h |
| Total living with HIV viral load done 12m |
2020 Q1 |
both sexes all ages DHIS-Tier |
3 499 427 |
364 948 |
184 411 |
903 853 |
1 086 030 |
296 396 |
418 580 |
17 862 |
227 347 |
|
a |
| 2021 Q1 |
both sexes all ages DHIS-Tier |
3 448 279 |
363 218 |
178 204 |
842 785 |
1 045 472 |
282 163 |
360 744 |
21 816 |
243 727 |
110 150 |
a |
| 2022 Q1 |
both sexes all ages DHIS |
3 984 279 |
402 455 |
218 952 |
939 513 |
1 237 379 |
320 189 |
436 061 |
27 607 |
278 937 |
123 186 |
a |
| Total living with HIV viral load suppressed 12m |
2020 Q1 |
both sexes all ages DHIS |
3 060 505 |
313 657 |
164 056 |
787 645 |
976 689 |
252 680 |
357 900 |
14 863 |
193 015 |
|
a |
| 2021 Q1 |
both sexes all ages DHIS |
3 035 283 |
318 804 |
158 778 |
744 538 |
925 390 |
246 225 |
316 453 |
17 781 |
209 772 |
97 542 |
a |
| 2022 Q1 |
both sexes all ages DHIS |
3 516 385 |
346 289 |
201 888 |
853 670 |
1 112 527 |
253 936 |
378 751 |
23 306 |
233 903 |
112 115 |
a |
Reference notes
a webDHIS.10
b UNAIDS 2021.61
c Stats SA MYE 2020.13
d Thembisa v4.4.62
e HIV and work 201863
f Thembisa v4.5.64
g UNAIDS Data 2020.65
h Stats SA MYE 2021.12
i Stats SA MYE 2022.11
j .Thembisa v4.3.66
k GBD 2017 HIV.67
Definitions
- Adult ART Total [Number].:
- Adult living with HIV [Number]: Estimated number of adults (15+ years) living with HIV.
- Adult living with HIV viral load done 12m [Number].
- Adult living with HIV viral load suppressed (VLS) 12m [Number]: ART client with suppressed viral load (VLS) of under 400 copies per millilitre (cps/mL).
- Adult remaining on ART at end of the month - total [Number].
- ART Adult client viral load done (VLD) [Number].
- ART Child client viral load done (VLD) [Number].
- Child ART Total [Number].
- Child living with HIV [Number]: Estimated number of children (0-14 years) living with HIV.
- Child living with HIV viral load done 12m [Number].
- Child living with HIV viral load suppressed (VLS) 12m [Number]: ART client with suppressed viral load (VLS) of under 400 copies per millilitre (cps/mL).
- Number of patients receiving ART [Number]: Number of patients receiving ART.
- People living with HIV (PLHIV) [Number]: The number of people who are HIV-positive.
- Total clients remaining on ART at the end of the month [Number].
- Total living with HIV [Number]: The estimated number of people who are HIV-positive.
- Total living with HIV viral load done 12m [Number].
- Total living with HIV viral load suppressed 12m [Number]: ART client with suppressed viral load (VLS) of under 400 copies per millilitre (cps/mL) at 12 months.
- Adult with viral load suppressed rate 12 months [Percentage]: Proportion of ART clients with viral load suppressed at different time intervals. This indicates the population level immunological impact of clients on ART.
- Antenatal client initiated on ART rate [Percentage]: Antenatal clients on ART as a proportion of the total number of antenatal clients who are HIV positive and not previously on ART.
- Antiretroviral coverage (2nd 90) [Percentage]: The number of patients receiving ART, divided by the number needing treatment. The denominator has changed over time, due to changes in treatment guidelines affecting the criteria for treatment eligibility. The latest definition is that all HIV-infected patients should be on ART. This indicator is also one of the 90-90-90 global targets for AIDS (UNAIDS).
- Antiretroviral effective coverage [Percentage]: Proportion of HIV-positive people on ART and virally suppressed. Any implausible values (>100) capped at 100, zero or missing values set to 1.
- ART client viral load suppressed rate (VLS) [Percentage]: ART viral load suppressed - total as a proportion of ART viral load done
- Child with viral load suppressed rate 12 months [Percentage]: Proportion of ART clients with viral load suppressed at different time intervals. This indicates the population level immunological impact of clients on ART.
- Clients remaining on ART rate [Percentage]: Percentage of estimated people living with HIV who remain on ART. (Routine data equivalent for antiretroviral coverage).
- HIV prevalence (age 15-49) [Percentage]: Percentage of population (age 15-49) estimated to be HIV-positive.
- HIV prevalence (total population) [Percentage]: Percentage of population estimated to be HIV-positive.
- HIV testing coverage [Percentage]: Percentage of target population who have been tested for HIV.
- HIV viral load suppression (3rd 90) [Percentage]: Percentage of people on ART who are virologically suppressed (VL level ≤1 000 copies/mL). This indicator is also one of the 90-90-90 global targets for AIDS (UNAIDS).
- Infant 1st PCR test positive at birth rate [Percentage]: Infants tested PCR positive for the first time at birth as proportion of infants PCR tested at birth.
- Medical male circumcision 15 years and older rate [Percentage]: Medical male circumcisions performed 15 years and older as a proportion of total medical male circumcisions performed.
- Percentage of deaths due to AIDS [Percentage]: Percentage of total deaths attributed to AIDS related causes.
- Percentage of people living with HIV (PLHIV) who know their status (1st 90) [Percentage]: Percentage of people living with HIV who know their HIV status. This indicator is also one of the 90-90-90 global targets for AIDS (UNAIDS).
The UNAIDS summary page on South Africa68 shows data for 2021, in the middle of the pandemic. Although new infections continued to decline, the rate at which HIV-related deaths were declining, slowed. These statistics provide the backdrop to the recently launched National Strategic Plan (NSP) for HIV, TB and STIs 2023-2028.69 Emphasis in the NSP 2023-2028 has been described as follows: “to provide innovative, people- and communities-centred interventions and multi-sectoral approaches to reduce the barriers and enhance access to equitable HIV, TB and STI prevention and treatment services”. This intent is closely aligned with the Global AIDS Strategy 2021-2026.70 However, policy objectives on paper do not translate easily into actionable interventions in the clinical setting. This was demonstrated in a cluster randomised controlled study conducted in 40 rural clinics in South Africa.71 Attempts to integrate HIV and TB services, with a quality-improvement component, failed to show an impact on mortality in HIV-TB co-infected patients. Even in sub-populations that have been the target of concerted effort over many years, such as pregnant women, reaching the third of the 95-95-95 targets has proven challenging.72 Table 19 shows the medical male circumcision (MMC) rates fluctuated between 2019/20 and 2021/22 which could have been the effect of some variations among the provinces where MMC rates went up quite drastically particularly between 2019/20 and 2020/21.
5.5. COVID-19
As the COVID-19 disease burden in South Africa and globally has reduced, so the frequency with which COVID-19 statistics are reported has dropped considerably. Although the dedicated COVID-19 website (https://sacoronavirus.co.za/) remains operative, it no longer gives daily statistics. Instead, the weekly COVID-19 reports now have to be accessed via the National Institute for Communicable Diseases (NICD) website (https://www.nicd.ac.za/diseases-a-z-index/disease-index-covid-19/surveillance-reports/). Most tellingly, the Daily Hospital Surveillance (DATCOV) reporting system is no longer functioning. This system had been highlighted as a prime example of collaboration between the public and private sectors, with 100% of all hospitals in each sector contributing data. The weekly DATCOV site only provides data until December 2022, and includes this note: “Please note: the DATCOV system ended at the end of December 2022 and COVID-19 hospitalisation data will be collected via the Notifiable Medical Conditions surveillance system from January 2023. These weekly COVID-19 hospitalisation reports have been discontinued from 31 December 2022.” Without weekly reporting, it is uncertain whether the COVID-19 hospitalisations are being consistently reported via the notifiable medical conditions (NMC) system. How many ambulatory cases are reported as NMCs is also uncertain. The rolling total on the South African coronavirus website showed 4 055 656 COVID-19 cases on 3 April 2023 and 102 595 deaths.
The weekly testing summary also ceased, from the end of March 2023 (epidemiological week 12 of 2023). The final report showed that 12 180 Polymerase Chain Reaction (PCR) tests were conducted in the week to 25 March 2022, bringing the cumulative national total to 21 577 962 since 1 March 2020.73 Interpreting the PCR percentage testing positive was no longer simple, as testing strategies varied between provinces. For example, settings in which all antigen-positive tests were confirmed by PCR would bias the statistic.
Although optional booster vaccinations are now accessible for all adults, uptake of COVID-19 vaccinations has slowed dramatically. Figures 18-20 show the vaccination statistics as at 20 February 2023. In March 2023, the WHO Strategic Advisory Group of Experts on Immunization (SAGE) revised its guidance.74 Additional booster doses were not recommended for healthy adults (those under the age of 50-60 years without comorbidities) and children and adolescents with comorbidities. Booster vaccination was still recommended for those at higher risk, namely older adults, younger adults with significant comorbidities (e.g. diabetes and heart disease), people with immune-compromised conditions (e.g. people living with HIV and transplant recipients; including children aged 6 months and older), pregnant persons, and frontline health workers. Children 5-11 years old at risk of severe disease became eligible for a primary course of vaccination from the end of February 2023.75

Figure 18.Total number of individuals vaccinated, by province, 20 February 2023
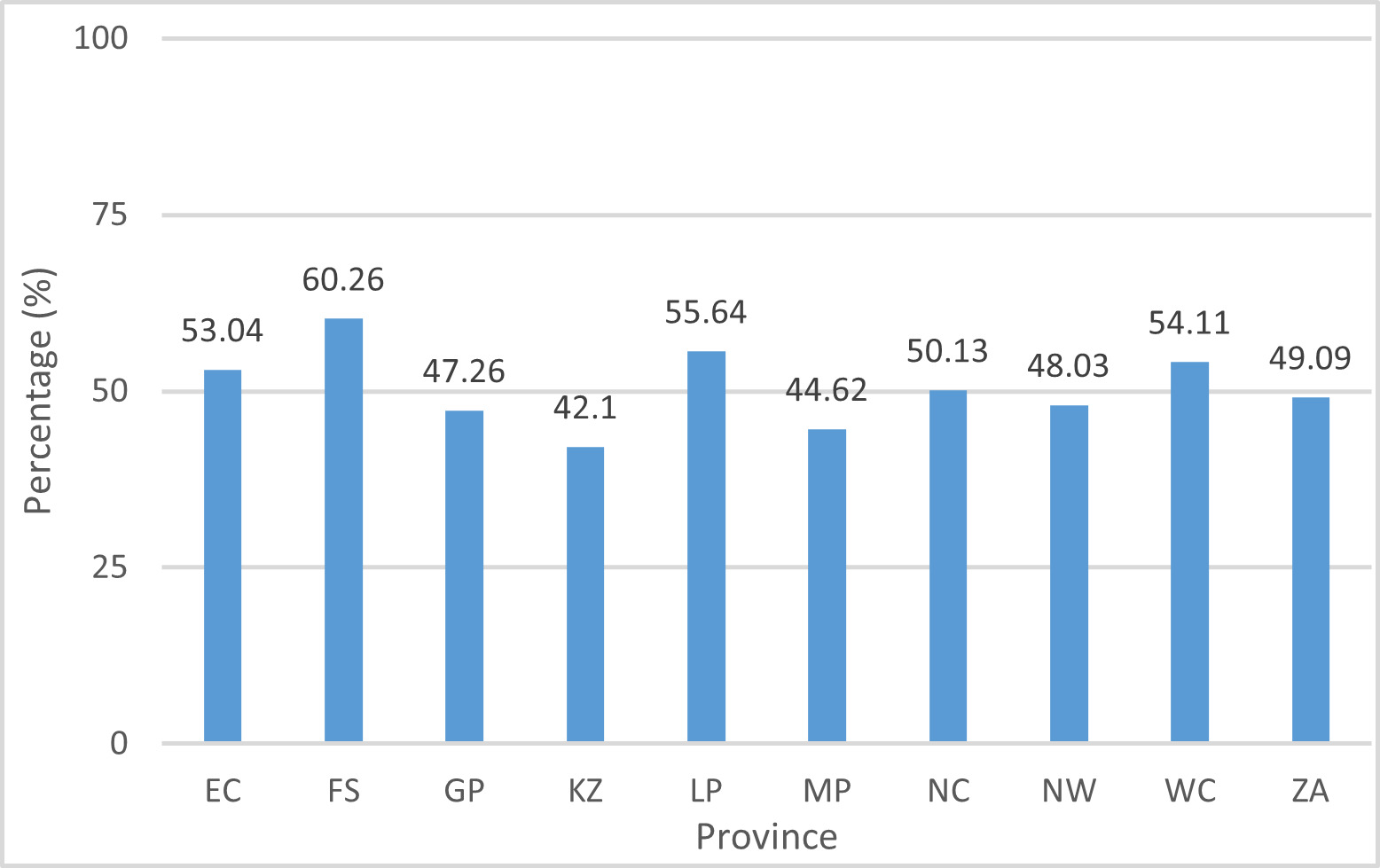
Figure 19.Individuals vaccinated as % of the population, 20 February 2023

Figure 20.Individuals vaccinated as % of the population by age group, 20 February 2023
5.6. Maternal and reproductive health
It has been found that during all pandemics, public focus shifts to preserving life, with less attention given to women, children, and reproductive health.76 The number of antenatal visits declined in all provinces during level 5 of the South African lockdown in 2020-2022 as illustrated in Figure 21 and Figure 22. All the provinces showed a significant increase in number of antenatal visits as lockdown levels lowered. All provinces, except for the Free State, experienced a drop in number of visits. This drop continued into the 2021/22 year, except in the Eastern Cape, where visits improved compared with the previous year, from 68.2% in 2020/21 to 81.2% in 2021/22. All provinces noted a reduction in the number of contraceptives methods prescribed (measured by the couple year protection rate) during lockdown levels 4 and 5; however, contraceptive prescription went back to usual as lockdown levels decreased (Figure 23 and Figure 24). All provinces showed an improvement in the couple year protection rate, except Gauteng, which declined from 44.9% in 2020/21 to 37.8% in 2021/22, and the Northern Cape which declined from 50.9% in 2020/21 to 46.8% in 2021/22 as shown in Table 14.
__january_2020_-_march_2022.png)
Figure 21.Antenatal 1st visit coverage (national), January 2020 - March 2022
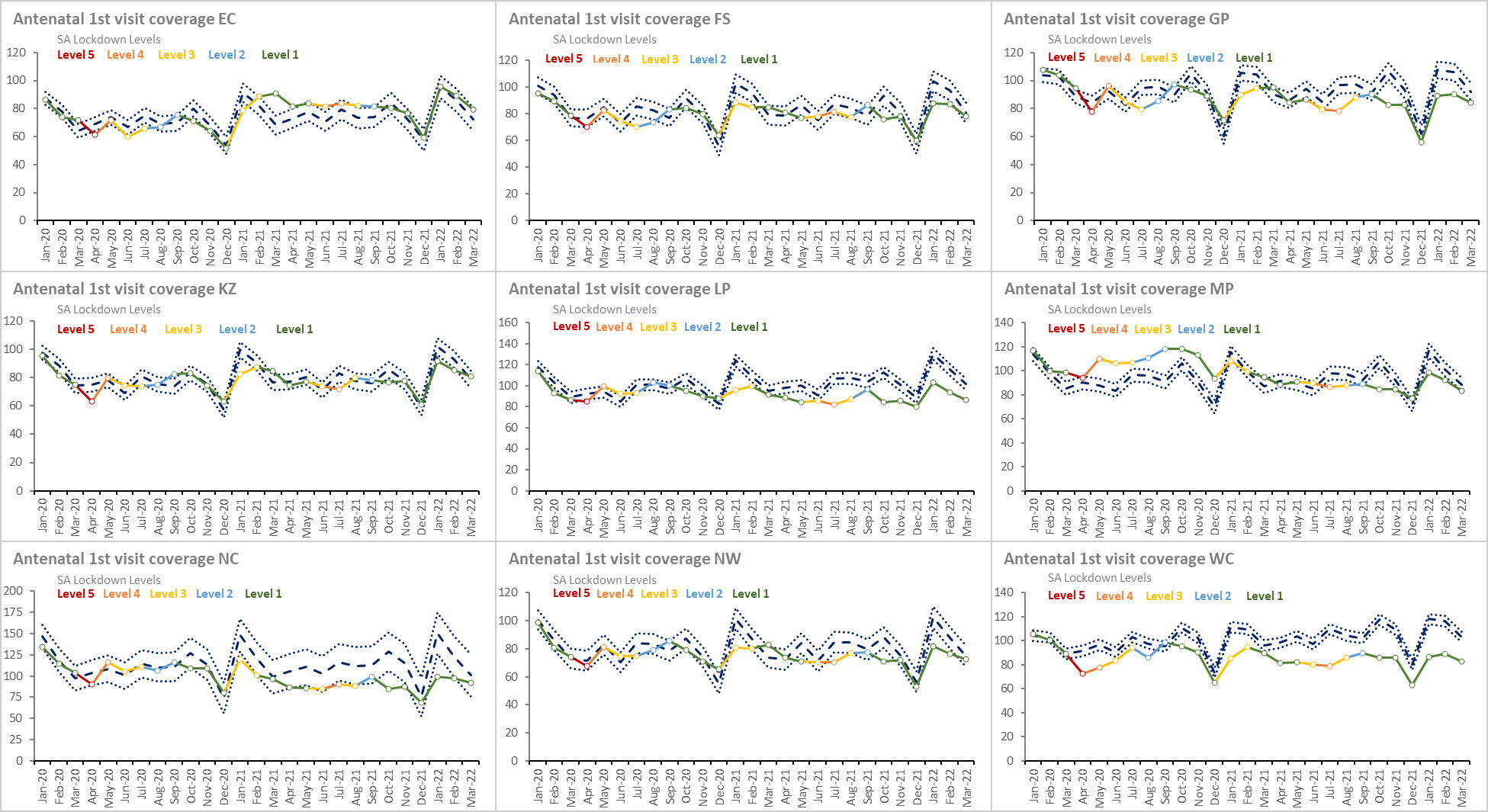
Figure 22.Antenatal 1st visit coverage per province, January 2020 – March 2022
__january_2020_-_march_2022.png)
Figure 23.Couple year protection rate (national), January 2020 - March 2022

Figure 24.Couple year protection rate per province, January 2020 – March 2022
Table 14.Maternal health indicators by province, 2018- 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Antenatal 1st visit before 20 weeks rate |
2019/20 |
female DHIS |
69,7 |
62,5 |
66,6 |
66,5 |
74,5 |
69,0 |
77,4 |
65,0 |
70,9 |
71,9 |
a |
| 2020/21 |
female DHIS |
67,9 |
62,5 |
61,3 |
63,3 |
74,6 |
66,8 |
74,9 |
58,6 |
68,0 |
70,6 |
a |
| 2021/22 |
female DHIS |
68,9 |
63,0 |
60,5 |
66,8 |
74,2 |
66,7 |
74,3 |
56,3 |
70,1 |
72,6 |
a |
| Antenatal 1st visit coverage |
2019/20 |
female DHIS |
83,1 |
68,7 |
79,3 |
90,2 |
75,0 |
90,7 |
92,7 |
105,6 |
77,7 |
91,1 |
a |
| 2020/21 |
female DHIS |
83,9 |
68,2 |
78,5 |
88,3 |
76,3 |
93,9 |
107,4 |
109,9 |
76,4 |
86,7 |
a |
| 2021/22 |
female DHIS |
81,5 |
81,2 |
78,9 |
82,5 |
77,3 |
88,0 |
87,6 |
88,6 |
72,1 |
82,6 |
a |
| Cervical cancer screening coverage |
2019/20 |
female DHIS |
46,8 |
50,0 |
46,0 |
42,2 |
55,9 |
33,3 |
57,9 |
32,0 |
55,9 |
41,8 |
a |
| 2020/21 |
female DHIS |
27,8 |
31,5 |
29,5 |
17,8 |
40,5 |
21,5 |
41,3 |
13,9 |
25,7 |
28,0 |
a |
| 2021/22 |
female DHIS |
36,9 |
32,9 |
35,2 |
31,4 |
56,8 |
25,1 |
42,7 |
15,3 |
22,8 |
40,0 |
a |
| Couple year protection rate |
2019/20 |
DHIS |
54,5 |
55,2 |
78,9 |
43,7 |
56,5 |
55,3 |
48,2 |
56,6 |
62,4 |
64,5 |
a |
| 2020/21 |
DHIS |
49,8 |
41,0 |
74,9 |
44,9 |
51,5 |
46,9 |
39,8 |
50,9 |
48,0 |
50,5 |
a |
| 2021/22 |
DHIS |
50,3 |
49,0 |
84,7 |
37,8 |
60,3 |
51,9 |
39,2 |
46,8 |
52,3 |
56,9 |
a |
| Delivery 10-14 years in facility |
2019/20 |
female DHIS |
3 870 |
671 |
192 |
631 |
704 |
447 |
618 |
134 |
149 |
324 |
a |
| 2021/22 |
female 10-14 years DHIS |
3 963 |
627 |
147 |
549 |
993 |
518 |
419 |
101 |
216 |
393 |
a |
| Delivery 10-19 years in facility |
2018/19 |
DHIS |
124 628 |
17 167 |
5 779 |
14 920 |
35 471 |
16 587 |
11 819 |
4 041 |
7 857 |
10 987 |
a |
| 2021/22 |
female 10-19 years DHIS |
139 361 |
18 960 |
6 647 |
20 877 |
35 820 |
18 070 |
14 425 |
3 976 |
9 424 |
11 162 |
a |
| Delivery 15-19 years in facility |
2019/20 |
female DHIS |
127 028 |
17 211 |
6 054 |
15 251 |
35 467 |
18 363 |
11 786 |
3 870 |
7 922 |
11 104 |
a |
| 2021/22 |
female 15-19 years DHIS |
135 398 |
18 333 |
6 500 |
20 328 |
34 827 |
17 552 |
14 006 |
3 875 |
9 208 |
10 769 |
a |
| Delivery by Caesarean section rate |
2019 |
female med schemes |
77,5 |
|
|
|
|
|
|
|
|
|
b |
| 2019/20 |
female DHIS |
29,0 |
30,9 |
31,8 |
31,2 |
33,7 |
21,4 |
22,4 |
21,5 |
25,0 |
29,9 |
a |
| 2020/21 |
female DHIS |
27,8 |
31,7 |
30,4 |
30,3 |
35,3 |
23,1 |
21,0 |
23,9 |
24,1 |
30,0 |
a |
| 2021/22 |
female DHIS |
29,6 |
32,3 |
32,3 |
30,6 |
36,4 |
23,2 |
20,3 |
22,2 |
23,4 |
30,9 |
a |
| Delivery by Caesarean section rate (district hospitals) |
2019/20 |
female DHIS District Hospital |
24,7 |
25,4 |
14,9 |
27,5 |
28,2 |
22,5 |
21,2 |
15,5 |
29,8 |
27,2 |
a |
| 2020/21 |
female DHIS District Hospital |
24,4 |
25,5 |
13,9 |
30,7 |
29,1 |
24,8 |
20,2 |
19,9 |
28,9 |
27,0 |
a |
| 2021/22 |
female DHIS District Hospital |
25,9 |
25,9 |
14,0 |
33,2 |
29,3 |
24,4 |
20,4 |
15,7 |
28,6 |
28,5 |
a |
| Delivery in 10 to 19 years in facility rate |
2019/20 |
female DHIS |
13,2 |
16,7 |
12,7 |
7,5 |
16,3 |
14,1 |
14,9 |
18,4 |
13,1 |
11,1 |
a |
| 2020/21 |
female DHIS |
14,3 |
17,1 |
13,1 |
8,9 |
16,5 |
13,8 |
15,5 |
19,3 |
14,0 |
10,8 |
a |
| 2021/22 |
female DHIS |
13,7 |
17,4 |
13,3 |
9,1 |
16,6 |
13,5 |
15,8 |
17,6 |
15,0 |
11,2 |
a |
| Delivery in facility rate |
2019/20 |
female DHIS |
79,3 |
61,4 |
87,5 |
75,2 |
78,4 |
94,9 |
88,1 |
98,4 |
72,9 |
89,5 |
a |
| 2020/21 |
female DHIS |
82,1 |
62,4 |
85,9 |
82,7 |
76,0 |
100,6 |
97,8 |
92,1 |
74,6 |
90,6 |
a |
| 2021/22 |
female DHIS |
83,3 |
77,8 |
92,7 |
81,5 |
79,0 |
100,2 |
88,2 |
82,0 |
72,6 |
84,6 |
a |
| Early neonatal death in facility rate |
2019/20 |
both sexes DHIS |
9,6 |
10,0 |
11,9 |
9,3 |
8,7 |
12,5 |
9,6 |
13,1 |
9,5 |
6,5 |
a |
| 2020/21 |
both sexes DHIS |
9,7 |
10,4 |
11,9 |
9,6 |
9,4 |
10,6 |
10,3 |
11,5 |
10,8 |
6,5 |
a |
| 2021/22 |
both sexes 0 DHIS |
10,0 |
10,3 |
12,6 |
10,5 |
9,8 |
10,7 |
10,5 |
10,3 |
11,1 |
6,1 |
a |
| Female condoms distributed |
2018/19 |
DHIS |
17 658 915 |
2 579 661 |
1 218 303 |
3 760 346 |
3 397 759 |
1 737 808 |
1 951 650 |
333 100 |
782 888 |
1 897 400 |
a |
| 2019/20 |
DHIS |
16 562 153 |
1 775 000 |
1 397 300 |
4 867 267 |
2 804 576 |
1 982 950 |
1 231 300 |
248 950 |
773 910 |
1 480 900 |
a |
| 2021/22 |
DHIS |
17 487 705 |
2 089 400 |
1 421 800 |
5 228 585 |
3 813 200 |
738 500 |
1 997 762 |
113 700 |
931 858 |
1 152 900 |
a |
| Live birth under 2500g in facility rate |
2019/20 |
both sexes DHIS |
12,9 |
14,1 |
14,2 |
13,9 |
11,7 |
10,6 |
11,6 |
18,9 |
13,6 |
13,9 |
a |
| 2020/21 |
both sexes DHIS |
13,2 |
13,6 |
14,4 |
13,0 |
11,8 |
10,7 |
11,5 |
16,7 |
13,3 |
13,6 |
a |
| 2021/22 |
both sexes 0 DHIS |
13,2 |
14,3 |
14,8 |
14,0 |
12,3 |
10,6 |
12,0 |
18,2 |
14,0 |
14,4 |
a |
| Male condom distribution coverage |
2019/20 |
DHIS |
32,1 |
34,7 |
52,3 |
25,1 |
30,1 |
35,5 |
32,8 |
28,9 |
38,7 |
33,2 |
a |
| 2020/21 |
DHIS |
26,5 |
22,3 |
50,9 |
26,3 |
26,6 |
27,5 |
23,9 |
23,8 |
27,4 |
21,4 |
a |
| 2021/22 |
DHIS |
26,1 |
22,4 |
56,1 |
21,1 |
29,0 |
28,3 |
19,1 |
20,9 |
28,1 |
27,3 |
a |
| Male condoms distributed |
2019/20 |
DHIS |
646 587 444 |
78 817 157 |
53 246 000 |
135 857 486 |
108 503 920 |
67 818 200 |
51 749 400 |
12 959 400 |
55 579 921 |
82 055 960 |
a |
| 2020/21 |
DHIS |
542 144 989 |
51 122 509 |
52 248 000 |
146 303 254 |
96 529 200 |
53 325 900 |
38 316 000 |
10 825 929 |
39 841 971 |
53 632 226 |
a |
| 2021/22 |
DHIS |
545 372 354 |
45 839 588 |
55 352 800 |
129 075 303 |
106 967 000 |
52 862 900 |
31 364 066 |
9 518 000 |
42 361 097 |
72 031 600 |
a |
| Maternal mortality in facility ratio |
2019/20 |
female DHIS |
88,0 |
108,2 |
116,2 |
102,9 |
76,9 |
97,8 |
67,1 |
109,9 |
88,0 |
43,6 |
a |
| 2020/21 |
female DHIS |
120,9 |
146,2 |
178,8 |
118,7 |
123,9 |
120,1 |
108,3 |
80,6 |
124,6 |
83,9 |
a |
| 2021/22 |
female DHIS |
119,1 |
114,6 |
156,5 |
129,3 |
100,6 |
134,6 |
130,0 |
157,5 |
129,9 |
75,1 |
a |
| Mother postnatal visit within 6 days rate |
2019/20 |
female DHIS |
80,1 |
69,0 |
80,5 |
85,5 |
76,1 |
104,2 |
70,9 |
68,6 |
93,2 |
60,1 |
a |
| 2020/21 |
female DHIS |
76,6 |
71,2 |
79,9 |
75,0 |
76,2 |
94,7 |
73,9 |
66,8 |
94,9 |
53,7 |
a |
| 2021/22 |
female DHIS |
78,6 |
78,6 |
76,6 |
74,7 |
79,3 |
95,2 |
74,2 |
61,1 |
102,6 |
57,1 |
a |
| Neonatal death in facility rate |
2019/20 |
both sexes DHIS |
11,9 |
12,3 |
15,6 |
12,4 |
10,9 |
14,3 |
11,2 |
15,5 |
11,5 |
8,2 |
a |
| 2020/21 |
both sexes DHIS |
12,6 |
13,1 |
16,0 |
13,2 |
12,1 |
12,7 |
12,7 |
13,8 |
13,9 |
8,3 |
a |
| 2021/22 |
both sexes DHIS |
13,1 |
13,2 |
15,9 |
14,3 |
13,0 |
13,2 |
12,9 |
12,9 |
14,6 |
7,7 |
a |
Neonatal mortality rate (NMR)
(deaths <28 days old per 1 000 live births) |
2018 |
both sexes WHO |
11,0 |
|
|
|
|
|
|
|
|
|
c |
| both sexes RMS |
11,0 |
|
|
|
|
|
|
|
|
|
d |
| 2019 |
both sexes WHO |
11,0 |
|
|
|
|
|
|
|
|
|
e |
| both sexes GBD |
20,7 |
|
|
|
|
|
|
|
|
|
f |
| 2020 |
both sexes WHO |
11,0 |
|
|
|
|
|
|
|
|
|
g |
| RMS |
12,0 |
|
|
|
|
|
|
|
|
|
h |
| Perinatal death in facility rate |
2019/20 |
both sexes DHIS |
29,1 |
29,0 |
35,4 |
27,9 |
29,7 |
31,7 |
28,2 |
36,8 |
31,0 |
22,9 |
a |
| 2020/21 |
both sexes DHIS |
29,8 |
31,3 |
38,7 |
29,1 |
32,7 |
30,9 |
13,3 |
33,9 |
33,9 |
24,6 |
a |
| 2021/22 |
both sexes DHIS |
30,8 |
30,3 |
38,6 |
29,5 |
32,3 |
29,5 |
31,1 |
43,6 |
33,2 |
24,1 |
a |
Perinatal mortality rate (stillbirths plus deaths
<8 days old per 1 000 total births) |
2018/19 |
both sexes DHIS |
30,1 |
28,3 |
39,9 |
28,6 |
30,8 |
31,7 |
30,2 |
34,3 |
30,6 |
25,6 |
a |
| 2019/20 |
both sexes DHIS |
25,0 |
18,8 |
32,7 |
24,3 |
24,5 |
32,0 |
26,5 |
37,9 |
23,9 |
21,7 |
a |
| 2021/22 |
both sexes DHIS |
27,2 |
25,4 |
38,1 |
25,4 |
27,3 |
31,1 |
29,0 |
38,0 |
24,8 |
21,6 |
a |
| Stillbirth in facility rate |
2019/20 |
both sexes DHIS |
19,7 |
19,2 |
23,8 |
18,8 |
21,2 |
19,5 |
18,8 |
24,0 |
21,7 |
16,5 |
a |
| 2020/21 |
both sexes DHIS |
19,9 |
21,1 |
27,1 |
19,7 |
23,6 |
20,5 |
3,0 |
22,6 |
23,4 |
18,3 |
a |
| 2021/22 |
both sexes DHIS |
21,0 |
20,1 |
26,3 |
19,2 |
22,8 |
19,0 |
20,8 |
33,6 |
22,4 |
18,1 |
a |
| Teenage pregnancy |
2021 |
female 14-19 years GHS |
2,7 |
|
|
|
|
|
|
|
|
|
i |
| ToPs (Terminations of Pregnancy) |
2019/20 |
DHIS |
124 446 |
12 597 |
7 776 |
23 048 |
27 441 |
14 960 |
8 127 |
1 497 |
9 806 |
19 194 |
a |
| 2020/21 |
DHIS |
103 350 |
9 696 |
6 888 |
22 832 |
21 754 |
13 660 |
2 494 |
1 454 |
8 367 |
16 205 |
a |
| 2021/22 |
DHIS |
120 144 |
13 107 |
7 837 |
26 427 |
24 204 |
14 408 |
6 706 |
1 816 |
9 222 |
16 417 |
a |
References
a webDHIS.10
b Medical Schemes 2019-20.77
c World Health Statistics 2020.78
d RMS 2018.45
e World Health Statistics 2021.31
f GBD 2021 Child Health.79
g World Health Statistics 2022.32
h RMS 2019 & 2021.46
i GHS 2021.18
Definitions
- Delivery 10-14 years in facility [Number]: Delivery where the mother is 10-14 years old. These deliveries are done in facilities under the supervision of trained medical/nursing staff.
- Delivery 10-19 years in facility [Number]: Delivery where the mother is 10-19 years old. These deliveries are done in facilities under the supervision of trained medical/nursing staff.
- Delivery 15-19 years in facility [Number]: Delivery where the mother is 15-19 years old. These deliveries are done in facilities under the supervision of trained medical/nursing staff.
- Female condoms distributed [Number]: Female condoms distributed from a primary distribution site to health facilities or points in the community (e.g. campaigns, non-traditional outlets, etc.).
- Male condoms distributed [Number]: Male condoms distributed from a primary distribution site to health facilities or points in the community (e.g. campaigns, non-traditional outlets, etc.).
- Maternal death in facility [Number]: Maternal death is death occurring during pregnancy, childbirth and puerperium within 42 days of termination of pregnancy, irrespective of the duration and site of pregnancy and the cause of death (obstetric and non-obstetric).
- Still birth in facility [Number]: Still born infants delivered in a health facility.
- ToPs (Terminations of Pregnancy) [Number]: The number of terminations of pregnancy.
- Antenatal 1st visit before 20 weeks rate [Percentage]: Women who have a booking visit (first visit) before they are 20 weeks (about half way) into their pregnancy as a proportion of all antenatal 1st visits.
- Antenatal 1st visit coverage [Percentage]: The proportion of pregnant women coming for at least one antenatal visit.
- Cervical cancer screening coverage [Percentage of target women]: Cervical smears in women 30 years and older as a proportion of the female population 30 years and older. 80% of these women should be screened for cervical cancer every 10 years and 20% must be screened every 3 years, which should be included in the denominator because it is estimated that 20% of women 30 years and older are HIV-positive.
- Couple year protection rate [Percentage]: Women protected against pregnancy by using modern contraceptive methods, including sterilisations, as proportion of female population 15-49 years.
- Delivery by Caesarean section rate (district hospitals) [Percentage]: Caesarean section deliveries, expressed as the proportion of total deliveries in facility
- Delivery in 10 to 19 years in facility rate [Percentage]: Deliveries to women under the age of 20 years as proportion of total deliveries in health facilities.
- Delivery in facility rate [Percentage]: Deliveries in health facilities as proportion of expected deliveries in the population.
- Early neonatal death in facility rate [per 1 000 live births]: Early neonatal deaths per 1 000 infants who were born alive in health facilities.
- Live birth under 2 500g in facility rate [Percentage]: Percentage of live births under 2 500g.
- Male condom distribution coverage [Condoms per male 15+]: Male condoms distributed from a primary distribution site to health facilities or points in the community (e.g. campaigns, non-traditional outlets, etc.).
- Maternal mortality in facility ratio [per 100 000 live births]: Women who die as a result of childbearing, during pregnancy or within 42 days of delivery or termination of pregnancy, per 100 000 live births, and where the death occurs in a health facility.
- Mother postnatal visit within 6 days rate [Percentage]: Mothers who received postnatal care within 6 days after delivery as proportion of deliveries in health facilities.
- Neonatal death in facility rate [per 1 000 live births]: Infants 0-28 days who died during their stay in the facility per 1000 live births in facility.
- Neonatal mortality in facility rate [per 1 000 live births]: Inpatient deaths within the first 28 days of life per 1 000 estimated live births. Estimated live births in population is calculated by multiplying estimated population under 1 year by 1.03 to compensate for infant mortality.
- Neonatal mortality rate (NMR) (deaths <28 days old per 1 000 live births) [per 1 000 live births]: Number of deaths within the first 28 days of life, in a year, per 1 000 live births during that year. Also called Neonatal Death Rate (NDR).
- Perinatal death in facility rate [per 1 000 total births]: Still births and deaths in facility under 7 days of life (Early Neonatal Death) per 1 000 births
- Perinatal mortality rate (stillbirths plus deaths <8 days old per 1 000 total births) [per 1 000 total births]: The number of perinatal deaths per 1 000 births. The perinatal period starts at the beginning of foetal viability (28 weeks’ gestation or 1 000g) and ends at the end of the 7th day after delivery. Perinatal deaths are the sum of stillbirths plus early neonatal deaths. These are divided by total births (live births plus stillbirths).
- Stillbirth in facility rate [per 1 000 births]: Stillbirths in facility per 1 000 total births in a facility.
- Teenage pregnancy [Percentage]: Percentage of women aged 15-19 who are mothers or who have ever been pregnant.
The crisis-management approach to the pandemic, which included lockdowns, school closures, and travel restrictions, placed women and adolescent girls at risk of having their rights violated, resulting in early pregnancy, gender-based violence, and lack of access to reproductive health services. The webDHIS figures in Table 14 show that deliveries by adolescents between the ages of 10 and 19 years increased across all provinces in 2021/22 compared to 2018/19. These findings underscore the importance of policies and programmes that provide life-skills training, financial literacy, support, and safe spaces for adolescent girls and women.80 There was also a significant increase in the maternal mortality ratio (MMR) in 2020/21 as noted in Table 14 where the MMR ranged from 178.8 in the Free State to 80.6 in the Northern Cape. This again points to the damaging effects of COVID-19 on maternal health.
There was a huge drop in cervical screening coverage between 2019/20 and 2021/21 due to COVID-19 and its effect on the national screening coverage programme. Cervical screening coverage rates were already low nationally at 46.8% and had still not recovered in 2021/22 (36.9%) yet cervical cancer is the second leading cause of cancer death among women following breast cancer.81
5.7. Child health
The global under-5-year mortality rate dropped to 37 deaths per 1 000 live births in 2020, but children in the African Region continued to have the highest mortality rates worldwide.32
Under-5 mortality (U5MR) continues to be one of the most challenging public health issues in LMICs, mainly due to poor dwelling units, poor access to breastfeeding, and the circumstances of birth, more specifically multiple births as these children are more likely to die than singleton children82 The leading causes of under-5 mortality are neonatal causes, diarrhoea, and pneumonia or lower respiratory tract infections, despite there being a high immunisation coverage rate and a decreasing occurrence of malnutrition.83 COVID-19 has resulted in a setback in achieving reduced deaths from infections and maternal and child health conditions that would have been possible by the year 2035. COVID-19 disrupted childhood vaccination programmes due to lockdowns, and redirected spending towards emergencies, including the procurement of COVID-19 vaccines.84
The monthly webDHIS figures (Figure 25 and Figure 26) indicate that immunisation coverage has stayed stable in the country, with a slight increase across all provinces except for North West in 2021/22. This could be due to the levels of lockdown having been gradually lifted at the time. The incidence of pneumonia cases decreased during higher levels of lockdown, driven in part by reduced care-seeking behaviours and patients only presenting for severe cases (Figure 27 and Figure 28). Figure 29 and Figure 30 show that cases of diarrhoea and dehydration also declined during higher levels of lockdown and increased slightly as restrictions were eased.
__january_2020_-_march_2023.png)
Figure 25.Immunisation under 1 year coverage (national), January 2020 - March 2023

Figure 26.Immunisation under 1 year coverage by province, January 2020 - March 2022
__january_2020_-_march_2022.png)
Figure 27.Child under 5 years pneumonia incidence (national), January 2020 - March 2022

Figure 28.Child under 5 years pneumonia incidence per province, January 2020 - March 2022
__january_2020_-_ma.png)
Figure 29.Diarrhoea with dehydration in child under 5 years incidence (national), January 2020 - March 2022

Figure 30.Diarrhoea with dehydration in child under 5 years incidence, per province, January 2020 - March 2022
Table 15.Child health indicators by province, 2018- 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| BCG coverage |
2020 |
UNICEF |
86,0 |
|
|
|
|
|
|
|
|
|
a |
| 2021 |
both sexes WHO/UNICEF |
86,0 |
|
|
|
|
|
|
|
|
|
b |
| 2020/21 |
both sexes DHIS |
88,4 |
68,0 |
93,2 |
102,5 |
73,0 |
93,2 |
98,7 |
106,7 |
65,3 |
94,9 |
c |
| 2021/22 |
both sexes DHIS |
87,6 |
84,6 |
96,1 |
95,0 |
83,7 |
93,5 |
84,7 |
88,3 |
55,6 |
97,2 |
c |
| Child under 5 years diarrhoea with dehydration incidence |
2018/19 |
both sexes DHIS |
7,1 |
4,9 |
9,2 |
5,9 |
7,9 |
8,0 |
2,7 |
8,5 |
5,6 |
14,0 |
c |
| 2019/20 |
both sexes DHIS |
7,0 |
6,5 |
8,7 |
5,8 |
8,0 |
6,9 |
1,3 |
9,4 |
6,4 |
11,9 |
c |
| 2021/22 |
both sexes DHIS |
7,3 |
7,2 |
7,7 |
6,4 |
6,6 |
7,3 |
5,9 |
9,3 |
3,6 |
14,6 |
c |
| Child under 5 years pneumonia incidence |
2019/20 |
both sexes DHIS |
23,6 |
10,3 |
32,2 |
16,8 |
28,9 |
14,2 |
4,0 |
27,7 |
8,4 |
80,8 |
c |
| 2020/21 |
both sexes DHIS |
12,6 |
5,5 |
13,1 |
10,5 |
11,6 |
5,8 |
3,3 |
12,3 |
3,4 |
48,1 |
c |
| 2021/22 |
both sexes DHIS |
19,1 |
8,7 |
19,9 |
13,7 |
17,6 |
8,9 |
5,1 |
16,7 |
4,0 |
82,0 |
c |
| Child under 5 years severe acute malnutrition incidence |
2019/20 |
both sexes DHIS |
1,9 |
0,8 |
5,9 |
1,5 |
1,9 |
1,1 |
0,8 |
8,3 |
4,3 |
1,7 |
c |
| 2020/21 |
both sexes DHIS |
1,5 |
1,3 |
4,1 |
1,1 |
1,3 |
1,5 |
0,7 |
5,6 |
2,1 |
1,0 |
c |
| 2021/22 |
both sexes DHIS |
2,0 |
2,0 |
5,5 |
1,6 |
1,6 |
2,2 |
1,0 |
6,1 |
2,7 |
1,3 |
c |
| Diarrhoea case fatality under 5 years rate |
2019/20 |
both sexes DHIS |
1,8 |
2,8 |
0,9 |
1,7 |
1,7 |
2,8 |
2,1 |
1,5 |
2,8 |
0,2 |
c |
| 2020/21 |
both sexes DHIS |
2,6 |
4,0 |
2,7 |
2,7 |
2,6 |
3,8 |
2,5 |
2,3 |
2,7 |
0,2 |
c |
| 2021/22 |
both sexes DHIS |
1,8 |
3,4 |
2,3 |
1,8 |
1,8 |
2,4 |
1,9 |
2,1 |
2,3 |
0,3 |
c |
| DTaP-IPV-Hib-HBV 3rd dose coverage |
2019/20 |
both sexes DHIS |
84,5 |
69,8 |
83,0 |
90,3 |
82,3 |
93,3 |
90,9 |
100,5 |
62,3 |
96,1 |
c |
| 2020/21 |
both sexes DHIS |
82,7 |
67,2 |
79,8 |
90,2 |
78,6 |
79,0 |
95,7 |
93,7 |
72,9 |
98,3 |
c |
| 2021/22 |
both sexes DHIS |
87,6 |
87,1 |
86,2 |
88,0 |
83,9 |
105,6 |
90,7 |
80,9 |
64,1 |
92,5 |
c |
| DTaP-IPV-Hib-HBV 4th dose coverage |
2018/19 |
both sexes DHIS |
65,5 |
56,2 |
61,3 |
67,9 |
68,2 |
66,5 |
67,1 |
74,7 |
55,8 |
71,8 |
c |
| 2019/20 |
both sexes DHIS |
65,5 |
59,4 |
63,8 |
68,2 |
65,6 |
65,9 |
70,5 |
78,1 |
47,3 |
75,7 |
c |
| 2021/22 |
both sexes DHIS |
69,5 |
69,3 |
70,2 |
69,9 |
71,3 |
72,9 |
66,2 |
62,4 |
49,0 |
80,0 |
c |
| DTP3 coverage |
2020 |
both sexes WHO |
84,0 |
|
|
|
|
|
|
|
|
|
d |
| 2021 |
both sexes WHO/UNICEF |
86,0 |
|
|
|
|
|
|
|
|
|
b |
| Immunisation under 1 year coverage |
2019/20 |
both sexes DHIS |
83,5 |
76,0 |
77,4 |
86,9 |
91,4 |
73,6 |
96,6 |
89,0 |
63,0 |
84,9 |
c |
| 2020/21 |
both sexes DHIS |
79,5 |
69,5 |
75,9 |
85,0 |
86,4 |
60,6 |
91,5 |
79,9 |
71,2 |
85,0 |
c |
| 2021/22 |
both sexes DHIS |
85,5 |
88,7 |
83,6 |
88,0 |
94,8 |
69,2 |
97,3 |
72,8 |
62,8 |
83,2 |
c |
| Infant mortality rate (deaths under 1 year per 1 000 live births) |
2019 |
RMS |
27,0 |
|
|
|
|
|
|
|
|
|
e |
| 2020 |
both sexes <1 year mid-year |
23,6 |
|
|
|
|
|
|
|
|
|
f |
| RMS |
21,0 |
|
|
|
|
|
|
|
|
|
e |
| 2021 |
both sexes mid-year |
24,1 |
|
|
|
|
|
|
|
|
|
g |
| Measles 1st dose under 1 year coverage |
2020 |
UNICEF |
84,0 |
|
|
|
|
|
|
|
|
|
a |
| 2021 |
both sexes WHO/UNICEF |
87,0 |
|
|
|
|
|
|
|
|
|
b |
| 2020/21 |
both sexes DHIS |
85,9 |
69,3 |
83,6 |
88,3 |
79,0 |
89,4 |
96,3 |
93,9 |
73,8 |
99,3 |
c |
| 2021/22 |
both sexes under 1 year DHIS |
88,5 |
88,1 |
89,6 |
88,8 |
84,0 |
95,6 |
97,8 |
81,8 |
73,5 |
94,5 |
c |
| Measles 2nd dose coverage |
2020 |
WHO/UNICEF |
76,0 |
|
|
|
|
|
|
|
|
|
h |
| 2021 |
both sexes WHO/UNICEF |
82,0 |
|
|
|
|
|
|
|
|
|
b |
| 2020/21 |
both sexes DHIS |
76,4 |
66,7 |
73,3 |
77,8 |
80,6 |
76,3 |
84,2 |
83,5 |
65,0 |
80,6 |
c |
| 2021/22 |
both sexes DHIS |
84,0 |
83,3 |
77,5 |
83,2 |
91,3 |
83,2 |
91,6 |
72,2 |
71,5 |
79,2 |
c |
| Number of under-5 deaths |
2019 |
GBD |
38 500 |
|
|
|
|
|
|
|
|
|
i |
| UNICEF |
41 000 |
|
|
|
|
|
|
|
|
|
a |
| OPV 1st dose coverage |
2020 |
UNICEF |
84,0 |
|
|
|
|
|
|
|
|
|
a |
| 2021/22 |
both sexes DHIS |
72,7 |
88,7 |
88,7 |
77,5 |
77,7 |
87,8 |
80,3 |
81,1 |
69,5 |
|
c |
| Orphanhood |
2021 |
both sexes <18 years GHS double |
2,4 |
3,9 |
3,0 |
1,5 |
3,2 |
2,4 |
1,9 |
1,6 |
0,8 |
1,7 |
c |
| both sexes <18 years GHS maternal |
2,2 |
2,3 |
2,7 |
1,6 |
2,8 |
2,1 |
3,1 |
2,9 |
2,6 |
0,9 |
c |
| both sexes <18 years GHS paternal |
7,0 |
9,0 |
8,0 |
5,8 |
7,6 |
5,3 |
7,4 |
4,6 |
8,8 |
6,2 |
c |
| PCV 3rd dose coverage |
2020 |
both sexes WHO |
83,0 |
|
|
|
|
|
|
|
|
|
d |
| 2021 |
both sexes WHO/UNICEF |
87,0 |
|
|
|
|
|
|
|
|
|
b |
| 2020/21 |
both sexes DHIS |
82,3 |
70,4 |
77,6 |
86,9 |
86,8 |
73,5 |
91,9 |
86,3 |
75,6 |
91,7 |
c |
| 2021/22 |
both sexes DHIS |
89,6 |
89,6 |
83,9 |
88,5 |
95,2 |
94,1 |
95,8 |
76,0 |
69,1 |
89,2 |
c |
| Pneumonia case fatality under 5 years rate |
2020/21 |
both sexes DHIS |
2,1 |
3,3 |
3,1 |
2,3 |
2,3 |
4,2 |
5,3 |
2,1 |
3,2 |
0,2 |
c |
| 2021/22 |
both sexes DHIS |
1,7 |
3,3 |
3,2 |
1,5 |
2,2 |
2,3 |
2,2 |
3,0 |
2,3 |
0,2 |
c |
| Pneumonia death under 5 years |
2019/20 |
both sexes DHIS |
806 |
139 |
44 |
116 |
192 |
154 |
66 |
24 |
42 |
29 |
c |
| 2020/21 |
both sexes DHIS |
621 |
98 |
26 |
98 |
148 |
109 |
74 |
16 |
32 |
20 |
c |
| 2021/22 |
both sexes DHIS |
690 |
117 |
44 |
98 |
196 |
89 |
36 |
40 |
44 |
26 |
c |
| RV 2nd dose coverage |
2020 |
UNICEF |
83,0 |
|
|
|
|
|
|
|
|
|
a |
| 2021 |
both sexes WHO/UNICEF |
85,0 |
|
|
|
|
|
|
|
|
|
b |
| 2020/21 |
both sexes DHIS |
83,2 |
67,4 |
78,7 |
91,4 |
77,5 |
71,2 |
97,7 |
93,1 |
76,4 |
95,3 |
c |
| 2021/22 |
both sexes DHIS |
86,7 |
87,2 |
87,7 |
88,7 |
83,3 |
92,7 |
92,7 |
80,5 |
69,9 |
90,4 |
c |
| Severe acute malnutrition case fatality under 5 years rate |
2019/20 |
both sexes DHIS |
7,8 |
9,9 |
6,0 |
6,4 |
7,6 |
7,9 |
10,6 |
4,7 |
11,8 |
1,5 |
c |
| 2020/21 |
both sexes DHIS |
7,3 |
8,6 |
3,2 |
7,7 |
10,5 |
8,0 |
16,0 |
5,0 |
4,9 |
2,2 |
c |
| 2021/22 |
both sexes under 5 years DHIS |
7,9 |
9,7 |
8,6 |
7,7 |
10,4 |
6,2 |
10,9 |
5,9 |
6,6 |
2,4 |
c |
| Under 5 mortality rate (deaths under 5 years per 1 000 live births) |
2020 |
both sexes WHO |
32,0 |
|
|
|
|
|
|
|
|
|
b |
| both sexes mid-year |
34,1 |
|
|
|
|
|
|
|
|
|
f |
| RMS |
28,0 |
|
|
|
|
|
|
|
|
|
e |
| 2021 |
both sexes mid-year |
30,8 |
|
|
|
|
|
|
|
|
|
g |
| Vaccine expenditure per population under 1 year |
2019/20 |
all programs real 2021/22 prices |
2 376 |
3 182 |
2 387 |
2 843 |
2 400 |
2 196 |
2 550 |
731 |
1 103 |
1 586 |
j |
| 2020/21 |
all programs real 2021/22 prices |
2 522 |
2 695 |
3 197 |
2 785 |
2 694 |
2 528 |
2 642 |
184 |
1 907 |
1 860 |
j |
| 2021/22 |
all programs real 2021/22 prices |
2 399 |
2 740 |
2 482 |
2 591 |
2 421 |
2 338 |
2 632 |
122 |
2 666 |
1 641 |
j |
Reference notes
a SWChildren 2021.47
b Immunization 2022.85
c webDHIS.10
d World Health Statistics 2022.32
e RMS 2019 & 2021.46
f Stats SA MYE 2020.13
g Stats SA MYE 2021.12
h Immunization 2021.86
i GBD 2021 Child Health.79
Definitions
- Number of under-5 deaths [Number]: The estimated number of deaths in children younger than 5 years.
- Pneumonia death under 5 years [Number]: A child under 5 years who died in a health facility where pneumonia was documented as the main cause of death
- BCG coverage [Percentage]: The proportion of expected live born babies that received BCG under 1 year of age (note: usually given immediately after birth).
- Child mortality (deaths between 1-4 years per 1 000 live births) [per 1 000 live births]: The number of children aged 12 months to 5 years (i.e. to the end of the 4th year) who die in a year, per 1 000 live births.
- Child under 5 years diarrhoea with dehydration incidence [Cases per 1 000 children]: Children under 5 years newly diagnosed with diarrhoea with dehydration per 1 000 children under 5 years in the population.
- Child under 5 years pneumonia incidence [Cases per 1 000 children]: Children under 5 years newly diagnosed with pneumonia per 1 000 children under 5 years in the population.
- Child under 5 years severe acute malnutrition incidence [Cases per 1 000 children]: Children under 5 years newly diagnosed with severe acute malnutrition per 1 000 children under 5 years in the population.
- Diarrhoea case fatality under 5 years rate [Percentage]: Diarrhoea deaths in children under 5 years as a proportion of diarrhoea separations under 5 years in health facilities.
- Diarrhoea incidence under 5 years [Cases per 1 000 children]: Children with diarrhoea per 1 000 children in the catchment population. Diarrhoea is formally defined as 3 or more watery stools in 24 hours, but any episode diagnosed and/or treated as diarrhoea after an interview with the adult accompanying the child.
- DTaP-IPV-Hib-HBV 3rd dose coverage [Percentage]: Children under 1 year who received DTaP-IPV-Hib-HBV 3rd dose, normally at 14 weeks as a proportion of population under 1 year. Both Pentaxim and Hexavalent will form part of the numerator to ensure accurate coverage of historical data.
- DTaP-IPV-Hib-HBV 4th dose coverage [Percentage]: Children under 2 years who received DTaP-IPV-Hib-HBV 4th dose, normally at 18 months as a proportion of the 1 year population. Both Pentaxim and Hexavalent will form part of the numerator to ensure accurate coverage of historical data.
- DTP3 coverage [Percentage]: The proportion of children who received their third DTP doses (normally at 14 weeks).
- Immunisation under 1 year coverage [Percentage]: The proportion of all children in the target area under one year who complete their primary course of immunisation. A Primary Course includes BCG, OPV 1, 2 & 3, DTP-Hib 1, 2 & 3, HepB 1, 2 & 3, and 1st measles (usually at 9 months).
- Infant mortality rate (deaths under 1 year per 1 000 live births) [per 1 000 live births]: The number of children less than one year old who die in a year, per 1 000 live births during that year.
- Measles 1st dose under 1 year coverage [Percentage]: Children under 1 year who received measles 1st dose, as a proportion of population under 1 year.
- Measles 1st to 2nd drop-out rate [Percentage]: The percentage of children who dropped out between the first and the second dose of the measles vaccine.
- Measles 2nd dose coverage [Percentage]: Children 1 year (12 months) who received measles 2nd dose, as a proportion of the 1 year population.
- OPV 1st dose coverage [Percentage]: The proportion of children under 1 immunised with OPV dose 1.
- Orphanhood [Percentage]: Proportion of children under 18 years whose biological mother, biological father or both parents have died.
- PCV 3rd dose coverage [Percentage]: Children under 1 year who received PCV 3rd dose, normally at 9 months as a proportion of population under 1 year.
- Percentage of children under 5 years of age with suspected pneumonia taken to a health facility [Percentage]: Percentage of children under 5 years of age with suspected pneumonia (cough and difficult breathing NOT due to a problem in the chest and a blocked nose) in the two weeks preceding the survey taken to an appropriate health facility or provider.
- Pneumonia case fatality under 5 years rate [Percentage]: Pneumonia deaths in children under 5 years as a proportion of pneumonia separations under 5 years in health facilities.
- Post-neonatal mortality rate (deaths 28-365 days age per 1 000 live births) [per 1 000 live births]: Number of deaths occurring between 28 and 365 days after birth per 1 000 live births in the same period.
- RV 2nd dose coverage [Percentage]: Children under 1 year who received RV 2nd dose as a proportion of children under 1 year.
- Severe acute malnutrition case fatality under 5 years rate [Percentage]: Severe acute malnutrition deaths in children under 5 years as a proportion of severe acute malnutrition (SAM) under 5 years in health facilities.
- Under 5 mortality rate (deaths under 5 years per 1 000 live births) [per 1 000 live births]: The number of children under 5 years who die in a year, per 1 000 live births during the year. It is a combination of the infant mortality rate, plus the age 1-4 mortality rate.
- Vaccine expenditure per population under 1 year [Rand per population U1 (real prices)]: Provincial expenditure on vaccines per population under 1 year.
5.8. Non-communicable diseases
In 2022 the NDoH published the National Strategic Plan for the Prevention and Control of Non-Communicable Diseases, 2022-202787 to fast-track their response towards the prevention and control of non-communicable diseases (NCDs), risk factors and mental conditions. This was also in recognition of the gaps that COVID-19 exposed in the delivery of NCD services as mortality and hospitalisation rates were much higher for those living with NCDs (both known and unknown) and among obese people in the country.88 The NSP proposed a cascade-based strategy similar to the 90-90-90 approach for HIV and AIDS, and TB. The proposed 90-60-50 cascade states that:
-
90% of all people over 18 will know whether or not they have raised blood pressure and/or raised blood glucose.
-
60% of people with raised blood pressure or blood glucose will receive intervention.
-
50% of people receiving interventions are controlled.87
NCD policies require increasingly efficient implementation as the attributable burden for diabetes mellitus is growing. For example, improved surveillance of risk factors, including physical activity, is crucial to improving NCD detection and response.89 A high mortality burden attributable to high systolic blood pressure underscores the need for improved care for hypertension and cardiovascular diseases, particularly stroke, to prevent morbidity and mortality.90
As mentioned before, South Africa’s population is ageing and those living with HIV are living longer due to the successful uptake of antiretroviral therapy (ART), which means that the NCD burden on the country will also increase as old age is a risk factor for developing an NCD. In 2022, Percept Actuaries & Consultants quantified the burden of NCDs in South Africa using datasets that included the General Household Survey, the National Income Dynamics Study (NiDS), the South Africa Demographic and Health Survey (2016/17), cause-of-death records, Council for Medical Schemes data, underwriting from insurers, National Health Accounts, and webDHIS data. Some key findings from the briefs were:
-
South African males were 1.38 times more likely than females to have diabetes. Among the medical scheme population, the odds of being male with hypertension were 1.17 times higher than the odds of being female with hypertension.
-
Objective measures of diabetes showed high prevalence of undiagnosed or poorly managed diabetes. Only 30% of men and women with diabetes reported that they had previously been diagnosed with diabetes.
-
Uncontrolled diabetes increased the risk of death among hospitalised COVID-19 patients; the risk of death was exacerbated in elderly males, and those who had co-morbidities such as hypertension, clotting disorders, cardiovascular disease and obesity.91
Data on NCDs continues to be difficult to find though, as NCDs are not notifiable medical conditions (NMC). However, there has been an improvement in this regard as cancer registries are being strengthened. Table 16 shows the cancer incidence rate in South Africa for 2020, as reported by the National Cancer Registry (NCR) by cancer type. The most prevalent cancers in the country are prostate, breast, cervical, lung and colorectal. Figure 31 illustrates the age-standardised incidence rates among males and females for cancers with the highest incidence in the country.
Table 16.Non-communicable disease indicators by province, 2019 - 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Diabetes client treatment new 18 - 44 years |
2020/21 |
both sexes DHIS |
259 093 |
45 278 |
3 076 |
44 351 |
9 835 |
90 762 |
27 866 |
4 137 |
30 251 |
3 537 |
a |
| 2021/22 |
both sexes DHIS |
187 508 |
22 584 |
2 305 |
39 389 |
9 410 |
85 658 |
10 535 |
4 837 |
9 246 |
3 544 |
a |
| Diabetes client treatment new 45 years and older |
2020/21 |
both sexes DHIS |
207 372 |
29 533 |
4 451 |
42 830 |
14 607 |
61 984 |
24 236 |
3 298 |
17 863 |
8 570 |
a |
| 2021/22 |
both sexes DHIS |
151 682 |
16 137 |
3 630 |
37 524 |
16 883 |
45 315 |
12 105 |
2 102 |
9 143 |
8 843 |
a |
| Diabetes new client 18 years and older detection rate |
2020/21 |
both sexes DHIS |
1,2 |
1,8 |
0,4 |
0,8 |
0,3 |
4,1 |
1,7 |
0,9 |
1,8 |
0,2 |
a |
| 2021/22 |
both sexes DHIS |
0,8 |
0,9 |
0,3 |
0,7 |
0,4 |
3,5 |
0,7 |
0,8 |
0,7 |
0,2 |
a |
| Diabetes prevalence |
2021 |
both sexes 20-79 years Diabetes Atlas |
11,3 |
|
|
|
|
|
|
|
|
|
b |
| Hypertension client treatment new 18-44 years |
2020/21 |
both sexes DHIS |
258 695 |
29 824 |
5 509 |
34 966 |
32 821 |
98 682 |
32 678 |
4 273 |
12 282 |
7 660 |
a |
| 2021/22 |
both sexes DHIS |
189 992 |
20 156 |
4 935 |
29 891 |
34 250 |
69 786 |
11 607 |
3 518 |
7 580 |
8 269 |
a |
| Hypertension client treatment new 45 years and older |
2020/21 |
both sexes DHIS |
274 116 |
33 934 |
11 341 |
61 379 |
21 811 |
63 485 |
35 112 |
8 014 |
18 139 |
20 901 |
a |
| 2021/22 |
both sexes DHIS |
222 870 |
22 422 |
9 208 |
61 842 |
24 707 |
44 469 |
20 105 |
8 734 |
9 902 |
21 481 |
a |
| Hypertension new client 18 years and older detection rate |
2020/21 |
both sexes DHIS |
1,30 |
1,50 |
0,90 |
0,90 |
0,80 |
4,40 |
2,20 |
1,50 |
1,10 |
0,60 |
a |
| 2021/22 |
both sexes DHIS |
1,00 |
1,00 |
0,70 |
0,80 |
0,80 |
3,00 |
1,00 |
1,40 |
0,60 |
0,60 |
a |
| Mental disorders treatment rate new |
2020/21 |
both sexes DHIS |
0,14 |
0,06 |
0,18 |
0,22 |
0,04 |
0,47 |
0,06 |
0,05 |
0,03 |
|
a |
| 2021/22 |
both sexes DHIS |
0,06 |
0,07 |
0,03 |
0,06 |
0,05 |
0,20 |
0,02 |
0,06 |
0,01 |
|
a |
| Mental Health Quotient |
2021 |
MHQ |
46,0 |
|
|
|
|
|
|
|
|
|
c |
| Mental health separation rate |
2019/20 |
DHIS |
2,8 |
2,2 |
10,5 |
1,2 |
2,5 |
2,1 |
1,3 |
1,6 |
1,7 |
3,5 |
a |
| 2021/22 |
both sexes DHIS |
3,8 |
2,4 |
20,1 |
1,9 |
2,3 |
2,4 |
1,7 |
1,5 |
1,9 |
4,3 |
a |
| Mortality between 30-70 years from cardiovascular, cancer, diabetes or chronic respiratory disease |
2019 |
both sexes WHO |
24,1 |
|
|
|
|
|
|
|
|
|
d |
| Suicide mortality rate (per 100 000 population) |
2019 |
both sexes WHO |
23,5 |
|
|
|
|
|
|
|
|
|
d |
Cancer incidence rate, by type of cancer
(per 100 000 population) |
2020 |
both sexes age-standardised NCR all cancers |
209,5 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR bladder |
4,3 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR breast |
52,6 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR cervix |
35,3 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR colorectal |
14,6 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR Corpus uteri |
8,0 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR karposi sarcoma |
6,1 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR Liver |
4,8 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR lung |
18,3 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR Ovary |
5,1 |
|
|
|
|
|
|
|
|
|
e |
| both sexes age-standardised NCR prostate |
68,3 |
|
|
|
|
|
|
|
|
|
e |
| female age-standardised NCR all cancers |
194,2 |
|
|
|
|
|
|
|
|
|
e |
| male age-standardised NCR all cancers |
242,1 |
|
|
|
|
|
|
|
|
|
e |
Reference notes
a webDHIS.10
b IDF Diabetes Atlas 2021.92
c MHQ 2021.93
d World Health Statistics 2022.32
e GLOBOCAN 2020.81
Definitions
- The MHQ provides an aggregate metric of wellbeing. An aggregate mental wellbeing score based on these aspects (the MHQ) positions individuals on a spectrum from Distressed to Thriving. The positive range of the scale represents the spectrum of normal functioning, and is a 200-point scale calibrated to a mean of 100 based on pre-pandemic responses in 2019, similar to the IQ scale. The negative range of the scale represents mental wellbeing scores associated with a negative impact on the ability to function and is associated with clinical level risks and challenges mental wellbeing (the MHQ) as well as multiple dimensional views.
- Diabetes client treatment new 18-44 years [Number]: Newly diagnosed clients 18-44 years with a fasting blood glucose of >7mmol/L or random blood glucose >11.1mol/L.
- Diabetes client treatment new 45 years and older [Number]: Newly diagnosed clients 45 years and older with a fasting blood glucose of >7mmol/L or random blood glucose >11.1mol/L.
- Diabetes prevalence [Percentage]: Percentage of people with diabetes.
- Hypertension client treatment new 18-44 years [Number]: Total number of new hypertension clients 18 - 44 years put on treatment.
- Hypertension client treatment new 45 years and older [Number]: Total number of new hypertension clients 45 years and older put on treatment.
- Age-standardised prevalence of non-raised blood pressure (index) [Scale 0-100]: Percentage of population 15 years and older with non-raised blood pressure, regardless of treatment status, age-standardised (Census 2011 population).
- Diabetes new client 18 years and older detection rate [Percentage]: Newly diagnosed clients 18 years and older with a fasting blood glucose of >7mmol/L or random blood glucose >11.1mol/L. initiated on treatment.
- Diabetes new client 40 years and older detection rate [Percentage]: Newly diagnosed clients with a fasting blood glucose of >7mmol/L or random blood glucose >11.1mol/L initiated on treatment.
- Hypertension new client 18 years and older detection rate [Percentage]: Newly diagnosed clients, >18 years, with a BP >140/90mmHg.
- Mental disorders treatment rate new [Percentage]: Clients treated for mental disorders (depression, anxiety, dementia, psychosis, mania, suicide, developmental disorders, behavioural disorders and substance use) as a proportion of total PHC headcount.
- Mental health admission rate [Percentage]: Proportion of clients admitted/separated for mental health problems. Inpatient separations are the total of day clients, inpatient discharges, inpatient deaths and inpatient transfers out.
- Mental health separation rate [Percentage]: Proportion of clients admitted for mental health problems. Inpatient separations is the total of inpatient discharges, inpatient deaths and inpatient transfers out.
- Mortality between 30-70 years from cardiovascular, cancer, diabetes or chronic respiratory disease [Percentage]: Unconditional probability of dying between exact ages 30 and 70 from any of cardiovascular disease, cancer, diabetes, or chronic respiratory disease.
- Suicide mortality rate (per 100 000 population) [per 100 000 population]: Suicide rate per 100 000 population in a specified period (age-standardised).
- Cancer incidence rate, by type of cancer (per 100 000 population) [per 100 000 population]: Number of new cancers of a specific site/type occurring per 100 000 population.
_incidence_rates_per_sex_for_highest-incidence_cancers_in_south_a.png)
Figure 31.Age-standardised (world) incidence rates per sex for highest-incidence cancers in South Africa, 2020
Source: Globocan, 2020.81
According to the International Disability Alliance’s report37 on COVID-19 and diabetes, diabetes was a strong risk factor for adverse COVID-19 outcomes; individuals with diabetes were more likely to be hospitalised or die as a result of COVID-19 infections than those not living with the disease. The International Diabetes Federation (IDF) 2021 Atlas92 estimated that South Africa has the highest number of people living with diabetes in Africa, with an estimate of 4.2 million people in 2021. Twelve years ago, in 2011, this figure was estimated at just 1.9 million. According to routine data collected in the webDHIS between 2020/21 and 2021/22, there were noticeable drops in the number of new diabetes and hypertension treatment clients in the public sector. This was another indication of potential under-screening and under-diagnosing due to disruptions to health services caused by COVID-19 (Table 16).
COVID-19 highlighted increasing concern around mental health, both globally and locally. The second annual Mental State of the World Report93 noted that mental wellbeing showed a greater decline in 2020 (8%) than in 2021 (3%). This correlates with the stringent COVID-19 measures taken by governments when the pandemic started, and directly correlates with the number of cases and deaths per million.93 The report further noted that the pandemic had the greatest effect on the mental well-being of younger generations worldwide, with 44% of 18-24-year-olds considered in the ‘Distressed’ or ‘Struggling’ range compared with only 7% of those aged 65 years and older. The Mental Health Quotient (MHQ) assessment “captures a comprehensive spectrum of emotional, social and cognitive attributes encompassing both problems (or symptoms) across 10 different mental health disorders (as defined by the DSM-5), as well as positive mental attributes. An aggregate mental wellbeing score based on these aspects (the MHQ) positions individuals on a spectrum from Distressed to Thriving.” South Africa and the UK had the lowest MHQ (a score of 46) among the 34 countries included in the assessment; according to the scale, this score was in the ‘Enduring’ range (Figure 32). Furthermore, South Africa stood out among all the other countries as the percentage of ‘Distressed’ or ‘Struggling’ increased by 8% from 28.55% in 2020 to 36% in 2021. Such indicators demonstrate the increasing need for comprehensive mental health action plans, and mental health programmes and services in the country.

Figure 32.Mental Health Quotient assessment score range
Source: Mental Health Million Project, 202293
5.9. Injuries and risk behaviours
In 2022, the Global Burden of Disease (GBD) alcohol group estimated the population-level risks of alcohol consumption by amount, geography, age, sex, and year. They recommended the development of tailored guidelines and recommendations on alcohol consumption by age and across regions due to the fact that existing low consumption thresholds were actually too high for younger populations. Additionally, the publication noted that young adult males are the highest consumers of alcohol globally, and interventions targeting them should be prioritised to minimise loss of health due to alcohol consumption.94
Research by the Alcohol Harms Reduction programme forecasts a marked reduction in alcohol-related health costs if legislative interventions increase the price of alcohol through minimum unit pricing, and if the availability of liquor is reduced by regulating outlet trading hours95
In South Africa, alcohol remains an important contributor to the overall disease burden, ranking fifth in terms of deaths and disability-adjusted life years (DALYs).96 In 2021, most alcohol and drug treatment and rehabilitation centres re-opened following closures during the height of the COVID-19 pandemic. The most recent report from the South African Community Epidemiology Network on Drug Use (SACENDU) covered both periods in 2021 (January-June, and July-December). It reported an increased number of admissions for alcohol and other drugs (AODs) in the second half of the year, from 10 938 (across 85 centres/programmes) to 15 704 (across 78 treatment centres/programmes) as shown in Table 17. There was a higher number of people seeking treatment for alcohol in the Western Cape and Gauteng, and a decline of 21% for such admissions in KwaZulu-Natal. Cannabis was the main drug of use among admissions aged 20 years and younger (Table 17).97
Table 17.Injury and risk behaviour indicators by province, 2018 -2021
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Mortality rate attributed to unintentional poisoning (per 100 000 population) |
2019 |
both sexes WHO |
1,7 |
|
|
|
|
|
|
|
|
|
a |
| Mortality rate due to homicides (per 100 000 population) |
2018 |
both sexes SAPS |
35,8 |
|
|
|
|
|
|
|
|
|
b |
| 2019 |
both sexes WHO |
35,9 |
|
|
|
|
|
|
|
|
|
a |
| Road accident fatalities |
2020 |
both sexes all ages RTMC |
9 969 |
1 336 |
647 |
1 855 |
2 031 |
1 161 |
1 046 |
265 |
720 |
908 |
c |
| Road accident fatalities per 100 000 population |
2018 |
both sexes all ages RTMC |
22,3 |
25 |
33 |
17 |
22 |
27 |
29 |
28 |
25 |
16 |
d |
| 2019 |
both sexes WHO |
22,2 |
|
|
|
|
|
|
|
|
|
a |
| both sexes all ages RTMC |
21,3 |
23,8 |
29,5 |
16,2 |
20,5 |
25,7 |
29,1 |
30,1 |
21,2 |
17,1 |
d |
| Prevalence of smoking |
2020 |
both sexes 15 years and older WHO |
20,3 |
|
|
|
|
|
|
|
|
|
a |
| Total alcohol per capita (age 15+ years) consumption (litres per year) |
2019 |
both sexes WHO |
9,5 |
|
|
|
|
|
|
|
|
|
a |
| Primary drug of abuse as % of all drugs of abuse |
Jan-Jun 2021 |
both sexes <20 years SACENDU alcohol |
|
12,0 |
|
10,8 |
8,2 |
|
|
|
|
9,5 |
e |
| both sexes <20 years SACENDU cannabis |
|
44,0 |
|
39,3 |
52,5 |
|
|
|
|
23,2 |
e |
| both sexes <20 years SACENDU cocaine |
|
4,0 |
|
3,2 |
1,9 |
|
|
|
|
0,4 |
e |
| both sexes <20 years SACENDU heroin |
|
0,0 |
|
22,2 |
19,6 |
|
|
|
|
18,3 |
e |
| both sexes <20 years SACENDU mandrax |
|
2,0 |
|
2,5 |
1,9 |
|
|
|
|
7,2 |
e |
| both sexes <20 years SACENDU methamphetamine |
|
14,0 |
|
12,7 |
8,2 |
|
|
|
|
39,5 |
e |
| Jul-Dec 2021 |
both sexes <20 years SACENDU alcohol |
|
3,3 |
|
4,1 |
1,5 |
|
|
|
|
2,8 |
e |
| both sexes <20 years SACENDU cannabis |
|
58,2 |
|
49,0 |
56,9 |
|
|
|
|
84,3 |
e |
| both sexes <20 years SACENDU cocaine |
|
|
|
0,6 |
8,4 |
|
|
|
|
0,2 |
e |
| both sexes <20 years SACENDU heroin |
|
|
|
16,1 |
14,1 |
|
|
|
|
0,6 |
e |
| both sexes <20 years SACENDU mandrax |
|
|
|
1,5 |
1,1 |
|
|
|
|
2,1 |
e |
| both sexes <20 years SACENDU methamphetamine |
|
38,5 |
|
21,7 |
10,7 |
|
|
|
|
8,5 |
e |
Reference notes
a World Health Statistics 2022.32
b SDG SA Report 2019.98
c Road Traffic Report 2020.99
d Road Traffic Report 2019.100
e SACENDU Phase 51.97
Definitions
- Road accident fatalities [Number]: Number of people killed during or immediately after a crash, or death within 30 days after a crash happened as a direct result of such crash.
- Mortality rate attributed to unintentional poisoning (per 100 000 population) [per 100 000]:
- Mortality rate due to homicides (per 100 000 population) [per 100 000]
- Road accident fatalities per 100 000 population [per 100 000 population]: Number of fatalities due to road accidents per 100 000 population. WHO Core indicator is mortality rate from road traffic injuries (per 100 000 population) defined as: Number of road traffic fatal injury deaths per 100 000 population (age-standardised).
- Prevalence of smoking [Percentage]: Proportion of population who currently smoke.
- Primary drug of abuse as % of all drugs of abuse [Percentage]: Percentage breakdown of the primary drug of abuse reported by patients admitted to treatment centres that are part of the SACENDU sentinel surveillance system.
6. Health service indicators
6.1. Health facilities
Figures 33 and 34 show the overall impact of the COVID-19 pandemic on health facility workload. Despite the direct workload associated with confirmed COVID-19 cases, the overall number of patient-day equivalents was below the predicted level until March 2022, as was in-patient bed utilisation (Figure 35 and Figure 36).
__january_2020_--_march_2022.png)
Figure 33.Patient-day equivalent (national), January 2020 – March 2022
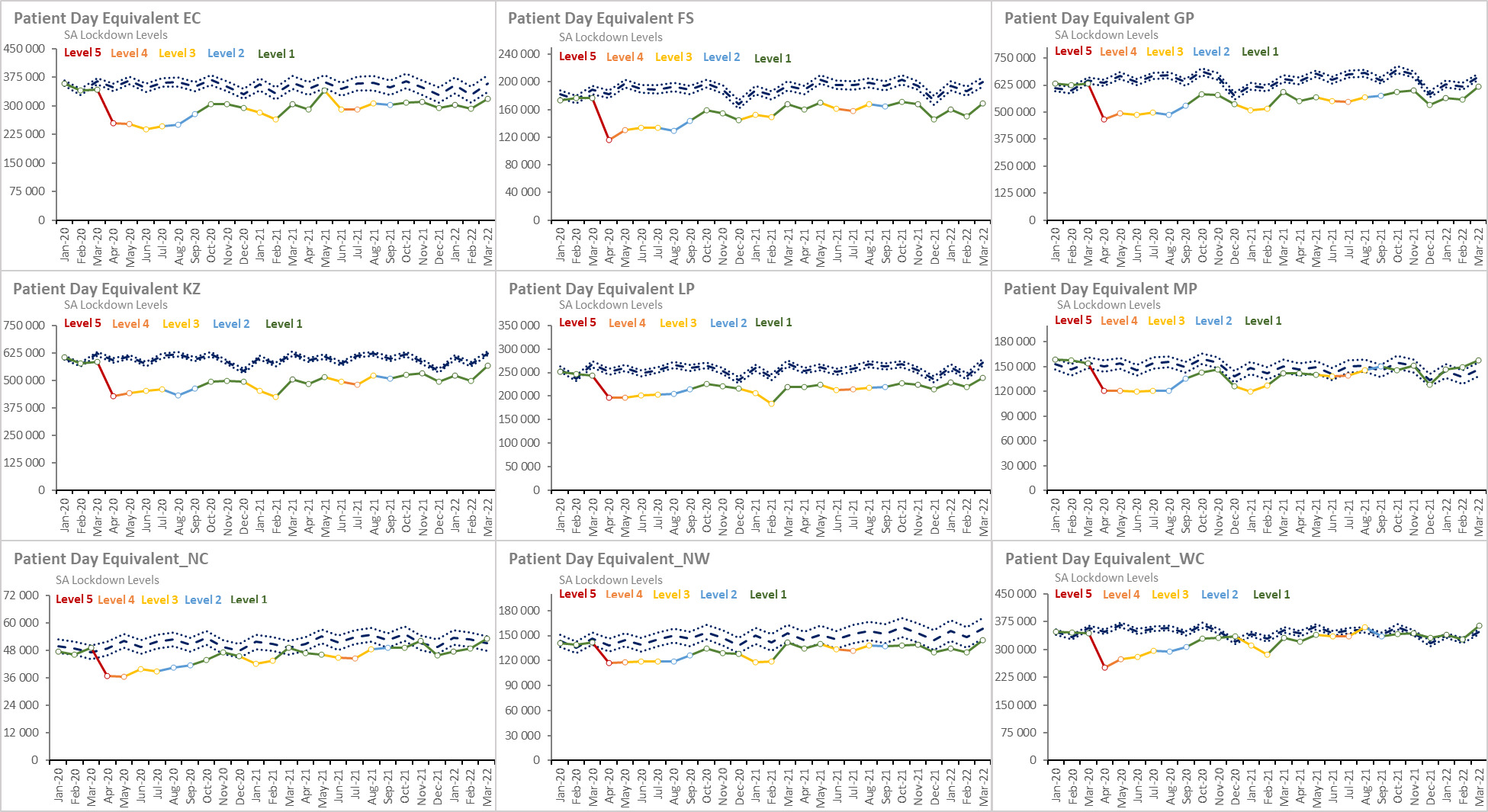
Figure 34.Patient-day equivalent by province, January 2020 – March 2022
__january_2020_--_march_2022.png)
Figure 35.Inpatient bed utilisation rate (national), January 2020 – March 2022

Figure 36.Inpatient bed utilisation rate by province, January 2020 – March 2022
The national bed utilisation rate (BUR) during the COVID-19 period dropped from 72.4% in 2019/20 to 60.7% but the average length of stay (ALOS) remained at 4 days. The inpatient crude death rate increased from 4.6% to 5.7% indicating that although less patients were admitted during the time, more patients probably died as a result of COVID-19. By contrast, primary health care (PHC) utilisation recovered to predicted levels over the same period, as shown in Figure 37 and Figure 38.
__january_2020_--_march_2022.png)
Figure 37.PHC utilisation rate (national), January 2020 – March 2022
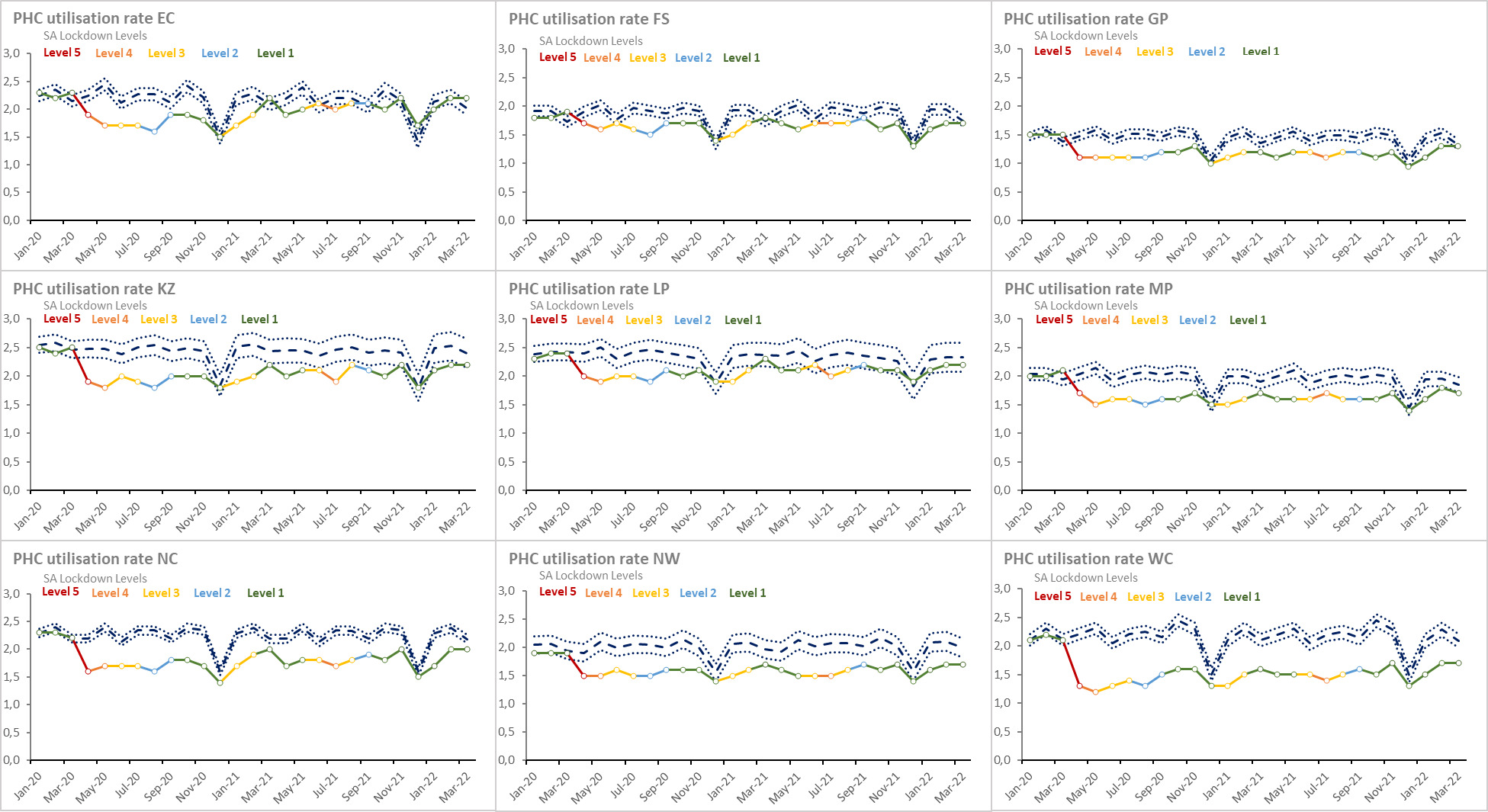
Figure 38.PHC utilisation rate by province, January 2020 – March 2022
Figure 39 to Figure 40, along with Table 18, show that the PHC utilisation rate for children under five is also on a steady recovery to pre-COVID levels in most provinces with the exception of the Northern Cape which had a PHC utilisation rate of 4.3 in 2019/20 and has only increased to 2.7 in 2021/22. Table 18 also illustrates how the total PHC headcount between 2019/20 and 2020/21 declined which resulted in less patients being seen by doctors and PHC professional nurses. This confirms the lack of essential services rendered to clients. The PHC headcount had still remained lower in the country in 2022 with only 101 393 994 people visiting PHCs compared to 2019 where it was estimated at close to 120 million people.
__january_2020_--_march_2022.png)
Figure 39.PHC utilisation under 5 years rate (national), January 2020 – March 2022

Figure 40.PHC utilisation under 5 years rate by province, January 2020 – March 2022
Table 18.Health services indicators by province, 2019 -2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Average length of stay - total |
2019/20 |
DHIS |
6,1 |
6,8 |
5,6 |
6,7 |
6,6 |
5,3 |
4,5 |
5,1 |
6,8 |
5,3 |
a |
| 2020/21 |
DHIS |
5,9 |
6,3 |
5,7 |
6,9 |
6,3 |
5,1 |
4,2 |
5,2 |
6,0 |
5,6 |
a |
| 2021/22 |
DHIS |
6,1 |
6,4 |
5,9 |
7,0 |
6,4 |
5,3 |
4,5 |
5,4 |
6,3 |
5,6 |
a |
| Average length of stay (district hospitals) |
2019/20 |
DHIS |
4,2 |
4,6 |
3,3 |
4,2 |
5,2 |
4,2 |
4,1 |
3,5 |
4,3 |
3,4 |
a |
| 2020/21 |
DHIS |
4,1 |
4,4 |
3,0 |
4,3 |
4,9 |
4,0 |
3,9 |
3,0 |
4,0 |
3,5 |
a |
| 2021/22 |
DHIS |
4,2 |
4,5 |
3,2 |
4,4 |
5,0 |
4,0 |
4,0 |
3,1 |
4,3 |
3,6 |
a |
| Complaints resolution rate |
2019/20 |
DHIS |
90,1 |
89,1 |
87,5 |
88,4 |
93,1 |
87,9 |
88,6 |
61,5 |
90,7 |
|
a |
| 2020/21 |
DHIS |
89,3 |
89,4 |
89,5 |
85,4 |
93,7 |
92,0 |
85,6 |
83,5 |
95,4 |
|
a |
| 2021/22 |
DHIS |
90,2 |
88,8 |
83,4 |
87,1 |
94,7 |
91,2 |
85,2 |
|
92,8 |
|
a |
| Complaints resolution rate within 25 working days |
2019/20 |
DHIS |
96,8 |
97,2 |
98,1 |
96,5 |
96,0 |
97,8 |
95,8 |
87,5 |
99,0 |
|
a |
| 2020/21 |
DHIS |
95,1 |
97,6 |
91,4 |
96,2 |
95,1 |
97,7 |
96,4 |
89,1 |
97,5 |
|
a |
| 2021/22 |
DHIS |
94,6 |
95,0 |
89,0 |
94,5 |
93,5 |
97,1 |
95,4 |
|
98,7 |
|
a |
| Death registration coverage |
2018 |
both sexes 15 years and older vital registration |
96,0 |
|
|
|
|
|
|
|
|
|
b |
| Inpatient bed utilisation rate - total |
2019/20 |
DHIS |
72,4 |
64,0 |
72,4 |
82,0 |
65,0 |
74,2 |
63,6 |
61,7 |
73,8 |
86,9 |
a |
| 2020/21 |
DHIS |
60,7 |
50,8 |
57,1 |
70,7 |
51,9 |
63,1 |
57,4 |
62,0 |
63,6 |
73,7 |
a |
| 2021/22 |
DHIS |
65,9 |
55,4 |
66,6 |
75,0 |
56,5 |
66,2 |
59,8 |
59,4 |
72,2 |
82,2 |
a |
| Inpatient bed utilisation rate (district hospitals) |
2019/20 |
DHIS |
64,8 |
54,5 |
57,7 |
70,2 |
59,2 |
72,9 |
67,0 |
53,6 |
62,8 |
90,4 |
a |
| 2020/21 |
DHIS |
53,6 |
42,2 |
47,0 |
59,9 |
47,6 |
60,9 |
57,0 |
48,8 |
52,7 |
78,5 |
a |
| 2021/22 |
DHIS |
57,3 |
46,0 |
51,5 |
63,7 |
50,2 |
62,6 |
58,7 |
43,4 |
59,3 |
90,0 |
a |
| Inpatient crude death rate |
2019/20 |
both sexes DHIS |
4,6 |
5,8 |
4,1 |
5,0 |
4,6 |
4,8 |
4,6 |
5,2 |
5,5 |
2,9 |
a |
| 2020/21 |
both sexes DHIS |
5,7 |
7,7 |
5,4 |
6,3 |
5,8 |
5,2 |
4,7 |
5,8 |
5,8 |
4,2 |
a |
| 2021/22 |
both sexes DHIS |
5,3 |
6,4 |
5,2 |
6,1 |
5,0 |
5,2 |
4,9 |
6,6 |
5,8 |
4,1 |
a |
| Inpatient deaths - total |
2019/20 |
both sexes DHIS |
179 752 |
27 472 |
12 904 |
40 064 |
35 920 |
19 216 |
11 922 |
4 306 |
10 134 |
17 814 |
a |
| 2020/21 |
both sexes DHIS |
188 814 |
30 103 |
13 068 |
41 296 |
37 118 |
18 340 |
11 642 |
3 950 |
10 802 |
22 495 |
a |
| 2021/22 |
both sexes DHIS |
187 531 |
27 206 |
13 829 |
42 653 |
33 879 |
18 500 |
11 912 |
4 914 |
10 964 |
23 674 |
a |
| International Health Regulations (IHR) core capacity index |
2019 |
WHO |
70,0 |
|
|
|
|
|
|
|
|
|
c |
| 2020 |
WHO |
79,0 |
|
|
|
|
|
|
|
|
|
d |
| 2021 |
both sexes WHO |
68,0 |
|
|
|
|
|
|
|
|
|
e |
| Number of beds |
Mar 2022 |
DHIS District Hospital |
30 904 |
6 040 |
1 600 |
2 806 |
4 265 |
3 006 |
8 297 |
588 |
1 235 |
3 067 |
a |
| DHIS National Central Hospital |
10 356 |
576 |
603 |
5 956 |
846 |
|
|
|
|
2 375 |
a |
| DHIS Provincial Tertiary Hospital |
10 194 |
1 772 |
588 |
2 254 |
1 586 |
1 016 |
799 |
661 |
1 236 |
282 |
a |
| DHIS Regional Hospital |
19 820 |
2 082 |
1 230 |
4 734 |
6 824 |
1 561 |
877 |
227 |
847 |
1 438 |
a |
| DHIS Specialised Psychiatric Hospital |
10 105 |
1 286 |
760 |
1 524 |
2 447 |
969 |
|
178 |
1 114 |
1 827 |
a |
| DHIS Specialised TB Hospital |
2 997 |
1 143 |
|
|
321 |
89 |
417 |
44 |
|
983 |
a |
| DHIS public sector |
88 556 |
13 186 |
6 525 |
17 836 |
7 900 |
5 099 |
20 897 |
1 895 |
4 432 |
10 786 |
a |
| Number of health facilities |
Mar 2022 |
DHIS District Hospital |
251 |
65 |
25 |
12 |
39 |
30 |
23 |
11 |
13 |
33 |
a |
| DHIS Central/Tertiary Hospital |
27 |
4 |
2 |
7 |
4 |
2 |
2 |
1 |
2 |
3 |
a |
| DHIS PHC fixed facilities |
3 505 |
776 |
220 |
373 |
618 |
482 |
295 |
162 |
312 |
267 |
a |
| DHIS Regional Hospital |
48 |
5 |
4 |
9 |
13 |
5 |
3 |
1 |
3 |
5 |
a |
| DHIS Other hospitals |
63 |
751 |
212 |
340 |
610 |
460 |
243 |
131 |
268 |
205 |
a |
| OHH headcount under 5 years coverage |
2019/20 |
DHIS |
86,8 |
67,1 |
53,8 |
60,6 |
160,3 |
84,1 |
54,6 |
126,0 |
138,7 |
0,0 |
a |
| 2020/21 |
DHIS |
69,7 |
35,2 |
39,8 |
52,3 |
118,3 |
100,2 |
27,5 |
82,2 |
51,4 |
120,7 |
a |
| 2021/22 |
DHIS |
95,0 |
48,5 |
74,2 |
67,6 |
145,3 |
117,9 |
63,1 |
74,1 |
72,7 |
134,3 |
a |
| OPD new client not referred rate |
2019/20 |
DHIS |
46,5 |
50,0 |
57,4 |
30,6 |
48,2 |
65,4 |
56,5 |
64,9 |
38,2 |
11,3 |
a |
| 2020/21 |
DHIS |
47,0 |
49,0 |
50,9 |
24,9 |
48,5 |
61,1 |
58,1 |
63,7 |
49,6 |
17,4 |
a |
| 2021/22 |
DHIS |
39,5 |
26,0 |
44,4 |
30,0 |
48,6 |
59,5 |
54,8 |
64,1 |
56,6 |
16,1 |
a |
| OPD new client not referred rate (district hospitals) |
2019/20 |
DHIS |
60,0 |
63,7 |
66,1 |
66,8 |
52,1 |
71,8 |
64,3 |
70,8 |
57,8 |
9,6 |
a |
| 2020/21 |
DHIS |
57,5 |
62,2 |
59,2 |
66,4 |
55,0 |
69,3 |
63,0 |
65,4 |
53,6 |
15,5 |
a |
| 2021/22 |
DHIS |
47,0 |
24,5 |
53,0 |
64,6 |
57,1 |
69,8 |
63,4 |
64,2 |
58,6 |
20,3 |
a |
| Patient Day Equivalent |
2019/20 |
DHIS |
32 461 949 |
4 295 480 |
2 172 659 |
7 521 238 |
7 100 648 |
3 010 254 |
1 869 054 |
579 169 |
1 676 989 |
4 236 460 |
a |
| DHIS District Hospital |
10 933 666 |
1 715 092 |
550 806 |
1 031 431 |
2 579 960 |
1 757 156 |
1 213 878 |
200 939 |
428 439 |
1 455 965 |
a |
| 2020/21 |
DHIS |
26 607 840 |
3 276 297 |
1 708 744 |
6 360 779 |
5 539 302 |
2 493 263 |
1 579 260 |
509 518 |
1 511 852 |
3 628 823 |
a |
| DHIS District Hospital |
8 969 900 |
1 345 068 |
457 235 |
855 601 |
2 085 569 |
1 442 600 |
997 636 |
163 152 |
395 338 |
1 227 700 |
a |
| 2021/22 |
DHIS |
29 679 714 |
4 083 839 |
1 946 643 |
6 834 424 |
6 139 074 |
2 659 570 |
1 733 190 |
577 039 |
1 630 542 |
4 075 393 |
a |
| DHIS District Hospital |
10 292 018 |
1 940 468 |
485 871 |
983 355 |
2 263 705 |
1 515 641 |
1 083 171 |
177 088 |
427 167 |
1 415 552 |
a |
| PHC doctor clinical work load |
2019/20 |
DHIS |
22,0 |
21,0 |
16,2 |
23,9 |
20,5 |
25,3 |
18,2 |
17,3 |
11,4 |
25,8 |
a |
| 2020/21 |
DHIS |
15,2 |
13,9 |
18,9 |
10,3 |
17,8 |
20,5 |
15,3 |
11,7 |
10,4 |
18,0 |
a |
| 2021/22 |
DHIS |
12,6 |
15,9 |
18,5 |
7,9 |
15,0 |
12,6 |
15,5 |
14,2 |
10,2 |
20,7 |
a |
| PHC heacount total |
2019/20 |
both sexes all ages DHIS |
119 747 336 |
16 420 094 |
5 303 035 |
21 309 158 |
28 353 937 |
14 347 755 |
9 220 716 |
2 728 252 |
7 714 952 |
14 349 437 |
a |
| 2020/21 |
both sexes all ages DHIS |
95 346 987 |
12 950 671 |
4 809 591 |
16 963 951 |
22 809 881 |
12 389 041 |
7 319 603 |
2 214 000 |
6 300 025 |
9 590 224 |
a |
| 2021/22 |
both sexes all ages DHIS |
101 393 994 |
13 692 661 |
4 771 693 |
18 647 814 |
23 906 112 |
12 752 688 |
7 734 010 |
2 333 065 |
6 605 539 |
10 950 412 |
a |
| PHC headcount 5 years and older |
2019/20 |
both sexes DHIS |
99 703 955 |
13 898 719 |
4 540 511 |
17 648 204 |
23 767 046 |
11 407 847 |
7 514 391 |
2 279 773 |
6 374 431 |
12 273 033 |
a |
| 2020/21 |
both sexes DHIS |
80 516 387 |
11 081 913 |
4 130 819 |
14 243 014 |
19 470 124 |
10 151 654 |
6 117 585 |
1 896 206 |
5 295 661 |
8 129 411 |
a |
| 2021/22 |
both sexes DHIS |
84 511 186 |
11 622 030 |
4 038 494 |
15 504 806 |
20 163 058 |
10 222 814 |
6 291 455 |
1 989 014 |
5 483 454 |
9 196 061 |
a |
| PHC headcount under 5 years |
2019/20 |
both sexes DHIS |
20 149 466 |
2 524 151 |
845 825 |
3 672 144 |
4 598 365 |
2 936 295 |
1 710 321 |
449 974 |
1 333 974 |
2 078 417 |
a |
| 2020/21 |
both sexes DHIS |
14 830 600 |
1 868 758 |
678 772 |
2 720 937 |
3 339 757 |
2 237 387 |
1 202 018 |
317 794 |
1 004 364 |
1 460 813 |
a |
| 2021/22 |
both sexes DHIS |
16 882 808 |
2 070 631 |
733 199 |
3 143 008 |
3 743 054 |
2 529 874 |
1 442 555 |
344 051 |
1 122 085 |
1 754 351 |
a |
| PHC professional nurse clinical work load |
2019/20 |
DHIS |
25,9 |
29,1 |
26,5 |
25,3 |
31,6 |
21,6 |
32,0 |
20,7 |
17,8 |
22,4 |
a |
| 2020/21 |
DHIS |
20,5 |
23,7 |
23,2 |
18,7 |
26,2 |
18,0 |
27,2 |
15,6 |
14,9 |
17,2 |
a |
| 2021/22 |
DHIS |
21,9 |
25,4 |
23,4 |
18,3 |
27,3 |
19,4 |
30,4 |
17,2 |
16,3 |
19,4 |
a |
| PHC utilisation rate |
2019/20 |
DHIS |
2,0 |
2,2 |
1,8 |
1,5 |
2,4 |
2,4 |
2,0 |
2,2 |
1,9 |
2,2 |
a |
| 2020/21 |
DHIS |
1,6 |
1,7 |
1,6 |
1,2 |
1,9 |
2,0 |
1,6 |
1,8 |
1,6 |
1,4 |
a |
| 2021/22 |
DHIS |
1,7 |
2,0 |
1,6 |
1,2 |
2,1 |
2,1 |
1,6 |
1,8 |
1,6 |
1,5 |
a |
| PHC utilisation rate under 5 years |
2019/20 |
DHIS |
3,4 |
3,0 |
3,1 |
2,9 |
3,5 |
4,4 |
3,9 |
4,3 |
3,4 |
3,8 |
a |
| 2020/21 |
DHIS |
2,6 |
2,7 |
2,6 |
2,1 |
2,7 |
3,4 |
2,6 |
2,5 |
2,5 |
2,6 |
a |
| 2021/22 |
DHIS |
3,0 |
3,0 |
2,8 |
2,4 |
3,0 |
3,9 |
3,0 |
2,7 |
2,8 |
3,1 |
a |
| Universal health coverage: service coverage index |
2021 |
GBD 2016 scaled |
49,4 |
|
|
|
|
|
|
|
|
|
f |
| 2022 |
GBD 2016 scaled |
50,5 |
|
|
|
|
|
|
|
|
|
f |
Reference notes
a webDHIS.10
b Stats SA Causes of Death 2018.101
c World Health Statistics 2020.78
d World Health Statistics 2021.31
e World Health Statistics 2022.32
f GBD 2016 SDGs.102
Definitions
- Inpatient deaths - total [Number]: An inpatient death is a death recorded against an admitted inpatient, including the death of a patient admitted earlier on the same day. The total is specialities plus all others that do not appear on the identified specialities.
- Number of beds [Number]: Total number of beds in health facility.
- Number of health facilities [Number].
- Patient Day Equivalent [Number]: The sum of Inpatient days total x 1, Day patient total x 0.5, and OPD/Emergency total headcount x 0.3333333.
- PHC headcount total [Number].
- PHC headcount 5 years and older [Number].
- PHC headcount under 5 years [Number]: All individual clients not yet reached five years (60 months) seen for Primary Health Care services at a facility.
- Average length of stay - total [Days]: The average number of patient days that an admitted patient spends in hospital before separation.
- Average length of stay (district hospitals) [Days]: The average number of patient days that an admitted patient spends in hospital before separation.
- Complaints resolution rate [Percentage]: Complaints resolved as a proportion of complaints received.
- Complaints resolution rate within 25 working days [Percentage]: Complaints resolved within 25 working days as a proportion of all complaints resolved.
- Death registration coverage [Percentage]: Percentage of deaths that are registered (with age and sex).
- Inpatient bed utilisation rate - total [Percentage]: A measure of the average number of beds that are occupied - expressed as the proportion of all available bed days, which is calculated as the number of actual beds multiplied by the average number of days in a month (30.42).
- Inpatient bed utilisation rate (district hospitals) [Percentage]: A measure of the average number of beds that are occupied - expressed as the proportion of all available bed days, which is calculated as the number of actual beds multiplied by the average number of days in a month (30.42).
- Inpatient crude death rate [Percentage]: Proportion of admitted clients/separations who died during hospital stay. Inpatient separations is the total of day clients, inpatient discharges, inpatient deaths and inpatient transfer outs.
- International Health Regulations (IHR) core capacity index [Percentage]: Percentage of attributes of 13 core capacities that have been attained at a specific point in time. The 13 core capacities are: (1) National legislation, policy and financing; (2) Coordination and National Focal Point communications; (3) Surveillance; (4) Response; (5) Preparedness; (6) Risk communication; (7) Human resources; (8) Laboratory; (9) Points of entry; (10) Zoonotic events; (11) Food safety; (12) Chemical events; (13) Radio-nuclear emergencies.
- OPD new client not referred rate [Percentage]: New OPD clients not referred as a proportion of OPD new clients – total.
- PHC doctor clinical work load [Clients per doctor per day]: Average number of clients seen per doctor per clinical work day. This includes doctors employed in the public and private sector.
- PHC professional nurse clinical work load [Clients per nurse per day]: Average number of clients seen per professional nurse per professional nurse clinical work day.
- PHC utilisation rate [Average number of visits per person]: Average number of PHC visits per person per year in the population.
- PHC utilisation rate under 5 years [Average number of visits per person under 5 years]: Average number of PHC visits per year per person under 5 years of age in the population.
- Universal health coverage: service coverage index [Scale 0-100]: Coverage of essential health services (defined as the average coverage of essential services based on tracer interventions that include reproductive, maternal, newborn and child health, infectious diseases, non-communicable diseases and service capacity and access, among the general and the most disadvantaged population). Calculated as the geometric mean of the index score for each of the 4 categories of the index.
6.2. Health personnel
The health personnel data provided in Table 19 and Table 20 only reflect those working in the public sector. The COVID-19 pandemic underscored the interrelatedness of the public and private health sectors, and enabled cross-sector service provision in one limited sense. The national COVID-19 vaccination programme was able to draw on the capacity of both sectors to deliver vaccine doses, regardless of insurance status. Changes to the reimbursement processes in early 2023 have reduced access to services in the private sector, with vaccine administration costs no longer reimbursed for uninsured persons.103
Table 19.Number of health personnel practising in the public sector by province, 2020 - 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Number of clinical associates |
2020 Mar |
both sexes public sector |
393 |
113 |
17 |
35 |
111 |
10 |
75 |
2 |
30 |
|
a |
| 2021 Mar |
both sexes public sector |
436 |
107 |
13 |
104 |
99 |
9 |
70 |
3 |
31 |
|
a |
| 2022 Mar |
both sexes public sector |
413 |
95 |
13 |
115 |
87 |
8 |
65 |
3 |
27 |
|
a |
| Number of CS clinical psychologists |
2020 Mar |
both sexes public sector |
66 |
3 |
3 |
39 |
7 |
3 |
0 |
1 |
3 |
7 |
a |
| 2021 Mar |
both sexes public sector |
54 |
1 |
3 |
28 |
4 |
2 |
3 |
1 |
5 |
7 |
a |
| 2022 Mar |
both sexes public sector |
69 |
3 |
2 |
34 |
14 |
2 |
2 |
2 |
3 |
7 |
a |
| Number of CS dentists |
2020 Mar |
both sexes public sector |
197 |
21 |
27 |
15 |
46 |
14 |
16 |
15 |
27 |
16 |
a |
| 2021 Mar |
both sexes public sector |
179 |
21 |
21 |
30 |
36 |
7 |
16 |
15 |
17 |
16 |
a |
| 2022 Mar |
both sexes public sector |
173 |
18 |
24 |
15 |
36 |
15 |
13 |
15 |
22 |
15 |
a |
| Number of CS dieticians |
2020 Mar |
both sexes public sector |
227 |
20 |
23 |
54 |
35 |
18 |
24 |
14 |
31 |
8 |
a |
| 2021 Mar |
both sexes public sector |
211 |
15 |
24 |
50 |
38 |
11 |
21 |
14 |
32 |
6 |
a |
| 2022 Mar |
both sexes public sector |
191 |
14 |
18 |
53 |
35 |
7 |
18 |
13 |
27 |
6 |
a |
| Number of CS doctors |
2020 Mar |
both sexes public sector |
1 527 |
160 |
62 |
253 |
252 |
165 |
209 |
76 |
149 |
201 |
a |
| 2021 Mar |
both sexes public sector |
1 700 |
169 |
105 |
287 |
269 |
158 |
235 |
75 |
190 |
212 |
a |
| 2022 Mar |
both sexes public sector |
2 137 |
219 |
94 |
417 |
391 |
220 |
303 |
97 |
194 |
202 |
a |
| Number of CS environmental health practitioners |
2020 Mar |
both sexes public sector |
182 |
3 |
23 |
43 |
4 |
47 |
15 |
13 |
34 |
|
a |
| 2021 Mar |
both sexes public sector |
103 |
1 |
5 |
24 |
3 |
30 |
14 |
8 |
18 |
|
a |
| 2022 Mar |
both sexes public sector |
195 |
3 |
20 |
39 |
7 |
49 |
21 |
12 |
44 |
|
a |
| Number of CS nurses |
2020 Mar |
both sexes public sector |
3 109 |
642 |
120 |
628 |
479 |
108 |
340 |
100 |
326 |
366 |
a |
| 2021 Mar |
both sexes public sector |
2 245 |
79 |
77 |
926 |
203 |
28 |
231 |
87 |
254 |
360 |
a |
| 2022 Mar |
both sexes public sector |
3 249 |
584 |
172 |
750 |
493 |
261 |
245 |
57 |
328 |
359 |
a |
| Number of CS occupational therapists |
2020 Mar |
both sexes public sector |
289 |
36 |
25 |
74 |
65 |
13 |
26 |
22 |
14 |
14 |
a |
| 2021 Mar |
both sexes public sector |
327 |
43 |
26 |
86 |
65 |
6 |
37 |
22 |
28 |
14 |
a |
| 2022 Mar |
both sexes public sector |
404 |
45 |
28 |
160 |
69 |
11 |
31 |
23 |
25 |
12 |
a |
| Number of CS pharmacists |
2020 Mar |
both sexes public sector |
612 |
66 |
45 |
91 |
134 |
67 |
48 |
40 |
83 |
38 |
a |
| 2021 Mar |
both sexes public sector |
653 |
68 |
48 |
92 |
149 |
65 |
51 |
46 |
96 |
38 |
a |
| 2022 Mar |
both sexes public sector |
636 |
71 |
72 |
80 |
150 |
70 |
49 |
36 |
66 |
42 |
a |
| Number of CS physiotherapists |
2020 Mar |
both sexes public sector |
352 |
35 |
29 |
94 |
73 |
8 |
36 |
24 |
29 |
24 |
a |
| 2021 Mar |
both sexes public sector |
383 |
41 |
29 |
95 |
72 |
17 |
35 |
29 |
42 |
23 |
a |
| 2022 Mar |
both sexes public sector |
323 |
54 |
23 |
24 |
89 |
16 |
27 |
26 |
38 |
26 |
a |
| Number of CS radiographers |
2020 Mar |
both sexes public sector |
367 |
29 |
17 |
94 |
81 |
24 |
34 |
14 |
37 |
37 |
a |
| 2021 Mar |
both sexes public sector |
364 |
24 |
13 |
107 |
83 |
19 |
37 |
17 |
28 |
36 |
a |
| 2022 Mar |
both sexes public sector |
355 |
30 |
15 |
113 |
78 |
21 |
33 |
15 |
14 |
36 |
a |
| Number of CS speech therapists |
2020 Mar |
both sexes public sector |
247 |
18 |
8 |
61 |
70 |
12 |
40 |
10 |
20 |
8 |
a |
| 2021 Mar |
both sexes public sector |
252 |
18 |
9 |
63 |
65 |
13 |
39 |
14 |
23 |
8 |
a |
| 2022 Mar |
both sexes public sector |
229 |
20 |
15 |
25 |
73 |
9 |
38 |
13 |
31 |
5 |
a |
| Number of dental practitioners |
2020 Mar |
both sexes public sector |
1 044 |
145 |
50 |
242 |
103 |
168 |
88 |
23 |
56 |
169 |
a |
| 2021 Mar |
both sexes public sector |
1 009 |
149 |
48 |
229 |
106 |
164 |
79 |
25 |
59 |
150 |
a |
| 2022 Mar |
both sexes public sector |
1 006 |
146 |
45 |
228 |
108 |
159 |
78 |
26 |
61 |
155 |
a |
| Number of dental specialists |
2020 Mar |
both sexes public sector |
152 |
1 |
1 |
113 |
|
2 |
1 |
1 |
|
33 |
a |
| 2021 Mar |
both sexes public sector |
126 |
1 |
1 |
89 |
1 |
4 |
1 |
1 |
|
28 |
a |
| 2022 Mar |
both sexes public sector |
128 |
|
1 |
88 |
1 |
4 |
1 |
1 |
|
32 |
a |
| Number of dental therapists |
2020 Mar |
both sexes public sector |
359 |
18 |
1 |
42 |
100 |
132 |
26 |
24 |
14 |
2 |
a |
| 2021 Mar |
both sexes public sector |
358 |
18 |
1 |
45 |
96 |
130 |
28 |
24 |
14 |
2 |
a |
| 2022 Mar |
both sexes public sector |
355 |
18 |
1 |
45 |
94 |
127 |
30 |
24 |
14 |
2 |
a |
| Number of enrolled nurses |
2020 Mar |
both sexes public sector |
29 638 |
3 321 |
1 033 |
7 188 |
8 939 |
3 591 |
1 639 |
238 |
962 |
2 727 |
a |
| 2021 Mar |
both sexes public sector |
32 191 |
4 145 |
1 224 |
7 961 |
9 710 |
3 195 |
1 467 |
268 |
1 267 |
2 954 |
a |
| 2022 Mar |
both sexes public sector |
31 775 |
3 502 |
1 231 |
7 810 |
10 016 |
3 151 |
1 548 |
253 |
1 225 |
3 039 |
a |
| Number of enrolled nurses registered |
2020 |
both sexes all ages SANC |
61 028 |
5 347 |
2 069 |
15 331 |
21 233 |
5 155 |
2 594 |
376 |
2 955 |
5 968 |
b |
| 2021 |
both sexes all ages SANC |
56 484 |
4 922 |
1 922 |
14 124 |
19 831 |
4 729 |
2 306 |
350 |
2 724 |
5 576 |
b |
| 2022 |
both sexes all ages SANC |
52 334 |
4 480 |
1 759 |
12 975 |
18 681 |
4 386 |
1 915 |
329 |
2 536 |
5 273 |
b |
| Number of environmental health practitioners |
2020 Mar |
both sexes public sector |
362 |
20 |
50 |
98 |
82 |
26 |
45 |
11 |
30 |
|
a |
| 2021 Mar |
both sexes public sector |
448 |
30 |
52 |
131 |
75 |
25 |
45 |
12 |
78 |
|
a |
| 2022 Mar |
both sexes public sector |
521 |
20 |
92 |
151 |
73 |
30 |
47 |
21 |
87 |
|
a |
| Number of medical practitioners |
2020 Mar |
both sexes public sector |
15 474 |
1 906 |
637 |
3 749 |
3 725 |
1 224 |
895 |
337 |
876 |
2 125 |
a |
| 2021 Mar |
both sexes public sector |
17 017 |
1 993 |
734 |
4 331 |
4 017 |
1 311 |
964 |
375 |
1 018 |
2 274 |
a |
| 2022 Mar |
both sexes public sector |
17 413 |
2 071 |
758 |
4 569 |
4 011 |
1 337 |
1 001 |
362 |
1 080 |
2 224 |
a |
| Number of medical researchers |
2020 Mar |
both sexes public sector |
33 |
2 |
2 |
14 |
5 |
2 |
|
1 |
|
7 |
a |
| 2021 Mar |
both sexes public sector |
32 |
2 |
2 |
16 |
5 |
1 |
|
1 |
|
5 |
a |
| 2022 Mar |
both sexes public sector |
128 |
4 |
|
16 |
90 |
9 |
1 |
1 |
|
7 |
a |
| Number of medical specialists |
2020 Mar |
both sexes public sector |
4 835 |
228 |
317 |
1 850 |
837 |
77 |
72 |
45 |
152 |
1 257 |
a |
| 2021 Mar |
both sexes public sector |
4 770 |
231 |
314 |
1 826 |
850 |
84 |
64 |
42 |
140 |
1 219 |
a |
| 2022 Mar |
both sexes public sector |
4 745 |
225 |
334 |
1 866 |
812 |
84 |
64 |
39 |
150 |
1 171 |
a |
| Number of nursing assistants |
2020 Mar |
both sexes public sector |
33 600 |
5 395 |
2 023 |
6 431 |
5 840 |
4 623 |
1 477 |
822 |
2 768 |
4 221 |
a |
| 2021 Mar |
both sexes public sector |
36 278 |
6 114 |
2 250 |
7 347 |
5 636 |
4 454 |
2 020 |
892 |
3 138 |
4 427 |
a |
| 2022 Mar |
both sexes public sector |
35 453 |
5 251 |
2 308 |
7 409 |
5 527 |
4 478 |
2 116 |
862 |
3 182 |
4 320 |
a |
| Number of nursing assistants registered |
2020 |
both sexes all ages SANC |
65 179 |
6 778 |
2 788 |
16 740 |
12 571 |
9 880 |
3 729 |
937 |
4 336 |
7 420 |
b |
| 2021 |
both sexes all ages SANC |
63 539 |
6 519 |
2 720 |
16 409 |
12 299 |
9 718 |
3 719 |
885 |
4 180 |
7 090 |
b |
| 2022 |
both sexes all ages SANC |
61 561 |
6 143 |
2 621 |
15 955 |
11 930 |
9 550 |
3 660 |
840 |
4 034 |
6 828 |
b |
| Number of occupational therapists |
2020 Mar |
both sexes public sector |
1 003 |
117 |
50 |
205 |
126 |
207 |
68 |
32 |
48 |
150 |
a |
| 2021 Mar |
both sexes public sector |
1 084 |
127 |
53 |
247 |
147 |
201 |
69 |
32 |
55 |
153 |
a |
| 2022 Mar |
both sexes public sector |
1 101 |
120 |
53 |
288 |
149 |
193 |
69 |
30 |
47 |
152 |
a |
| Number of optometrists and opticians |
2020 Mar |
both sexes public sector |
255 |
8 |
5 |
55 |
60 |
111 |
7 |
2 |
5 |
2 |
a |
| 2021 Mar |
both sexes public sector |
256 |
6 |
5 |
54 |
65 |
111 |
7 |
2 |
5 |
1 |
a |
| 2022 Mar |
both sexes public sector |
257 |
6 |
6 |
57 |
63 |
109 |
7 |
2 |
5 |
2 |
a |
| Number of pharmacists |
2020 Mar |
both sexes public sector |
5 337 |
865 |
315 |
1 169 |
813 |
520 |
304 |
103 |
259 |
989 |
a |
| 2021 Mar |
both sexes public sector |
5 543 |
912 |
331 |
1 251 |
818 |
521 |
332 |
114 |
264 |
1 000 |
a |
| 2022 Mar |
both sexes public sector |
5 777 |
887 |
406 |
1 280 |
851 |
583 |
355 |
104 |
284 |
1 027 |
a |
| Number of physiotherapists |
2020 Mar |
both sexes public sector |
1 110 |
147 |
48 |
194 |
244 |
158 |
76 |
31 |
71 |
141 |
a |
| 2021 Mar |
both sexes public sector |
1 239 |
155 |
51 |
245 |
280 |
159 |
78 |
31 |
80 |
160 |
a |
| 2022 Mar |
both sexes public sector |
1 225 |
144 |
53 |
250 |
274 |
164 |
79 |
31 |
70 |
160 |
a |
| Number of professional nurses |
2020 Mar |
both sexes public sector |
70 437 |
11 091 |
2 104 |
14 001 |
16 772 |
9 109 |
5 799 |
1 491 |
4 846 |
5 224 |
a |
| 2021 Mar |
both sexes public sector |
76 485 |
11 672 |
2 498 |
15 527 |
18 699 |
9 201 |
6 234 |
1 588 |
5 394 |
5 672 |
a |
| 2022 Mar |
both sexes public sector |
76 293 |
10 953 |
2 676 |
16 323 |
18 827 |
8 778 |
6 270 |
1 511 |
5 369 |
5 586 |
a |
| Number of professional nurses registered |
2020 |
both sexes all ages SANC |
154 024 |
16 620 |
8 267 |
40 200 |
35 470 |
13 457 |
8 647 |
2 382 |
10 780 |
18 201 |
b |
| 2021 |
both sexes all ages SANC |
156 392 |
16 661 |
8 398 |
41 183 |
35 807 |
13 659 |
8 889 |
2 383 |
10 947 |
18 465 |
b |
| 2022 |
both sexes all ages SANC |
157 152 |
16 643 |
8 412 |
41 761 |
35 569 |
13 701 |
9 156 |
2 379 |
11 017 |
18 514 |
b |
| Number of psychologists |
2020 Mar |
both sexes public sector |
637 |
67 |
27 |
191 |
61 |
120 |
32 |
15 |
43 |
81 |
a |
| 2021 Mar |
both sexes public sector |
705 |
69 |
30 |
224 |
74 |
115 |
48 |
16 |
49 |
80 |
a |
| 2022 Mar |
both sexes public sector |
780 |
65 |
29 |
243 |
94 |
132 |
48 |
16 |
48 |
105 |
a |
| Number of pupil auxiliary nurses registered |
2020 |
both sexes all ages SANC |
1 921 |
357 |
76 |
881 |
275 |
21 |
39 |
115 |
60 |
97 |
b |
| 2021 |
both sexes all ages SANC |
1 156 |
204 |
71 |
443 |
166 |
11 |
21 |
112 |
48 |
80 |
b |
| 2022 |
both sexes all ages SANC |
1 456 |
251 |
76 |
647 |
163 |
16 |
21 |
112 |
59 |
111 |
b |
| Number of pupil nurses registered |
2020 |
both sexes all ages SANC |
2 579 |
179 |
78 |
1 243 |
723 |
64 |
51 |
0 |
60 |
181 |
b |
| 2021 |
both sexes all ages SANC |
1 513 |
94 |
59 |
719 |
420 |
52 |
35 |
|
6 |
128 |
b |
| 2022 |
both sexes all ages SANC |
1 468 |
78 |
58 |
714 |
399 |
52 |
33 |
|
6 |
128 |
b |
| Number of radiographers |
2020 Mar |
both sexes public sector |
2 716 |
375 |
147 |
650 |
600 |
198 |
119 |
74 |
113 |
440 |
a |
| 2021 Mar |
both sexes public sector |
2 882 |
397 |
160 |
737 |
611 |
201 |
121 |
77 |
124 |
454 |
a |
| 2022 Mar |
both sexes public sector |
3 034 |
382 |
178 |
878 |
609 |
216 |
125 |
73 |
125 |
448 |
a |
| Number of speech therapists and audiologists |
2020 Mar |
both sexes public sector |
502 |
47 |
9 |
131 |
92 |
69 |
39 |
15 |
27 |
73 |
a |
| 2021 Mar |
both sexes public sector |
600 |
57 |
10 |
161 |
146 |
64 |
43 |
15 |
31 |
73 |
a |
| 2022 Mar |
both sexes public sector |
617 |
53 |
11 |
161 |
152 |
72 |
44 |
16 |
31 |
77 |
a |
| Number of student nurses |
2020 Mar |
both sexes public sector |
2 765 |
|
|
1 593 |
458 |
155 |
552 |
|
7 |
|
a |
| 2021 Mar |
both sexes public sector |
1 712 |
|
|
691 |
472 |
134 |
414 |
|
1 |
|
a |
| 2022 Mar |
both sexes public sector |
968 |
|
|
43 |
537 |
19 |
366 |
|
3 |
|
a |
| Number of student nurses registered |
2020 |
both sexes all ages SANC |
19 084 |
3 962 |
1 350 |
4 434 |
2 431 |
1 509 |
578 |
264 |
1 825 |
2 731 |
b |
| 2021 |
both sexes all ages SANC |
15 469 |
3 324 |
1 068 |
3 695 |
1 942 |
1 147 |
399 |
183 |
1 624 |
2 087 |
b |
| 2022 |
both sexes all ages SANC |
14 836 |
3 011 |
1 034 |
3 507 |
1 993 |
1 066 |
489 |
167 |
1 542 |
2 027 |
b |
Reference notes
a PERSAL.104
Table 20.Health personnel per 100 000 uninsured population by province, 2020 - 2022
| Indicator |
Period |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Clinical Associates per 100 000 population |
2020 Mar |
0,8 |
1,9 |
0,7 |
0,3 |
1,1 |
0,2 |
1,8 |
0,2 |
0,8 |
|
a |
| 2021 Mar |
0,9 |
1,8 |
0,5 |
0,9 |
1,0 |
0,2 |
1,7 |
0,3 |
0,8 |
|
a |
| 2022 Mar |
0,8 |
1,6 |
0,5 |
0,9 |
0,8 |
0,1 |
1,5 |
0,3 |
0,7 |
|
a |
| Density of dentistry personnel (per 10 000 population) |
2012-2020 |
1,1 |
|
|
|
|
|
|
|
|
|
b |
| Density of midwifery personnel (per 10 000 population) |
2012-2020 |
49,7 |
|
|
|
|
|
|
|
|
|
b |
| Density of pharmaceutical personnel (per 10 000 population) |
2012-2020 |
2,7 |
|
|
|
|
|
|
|
|
|
b |
| Density of physicans (per 10 000 population) |
2010-2018 |
9,1 |
|
|
|
|
|
|
|
|
|
b |
| 2012-2020 |
7,9 |
|
|
|
|
|
|
|
|
|
b |
| Dental practitioners per 100 000 population |
2020 Mar |
2,5 |
2,7 |
3,1 |
2,2 |
1,5 |
3,2 |
2,5 |
3,5 |
2,3 |
3,3 |
a |
| 2021 Mar |
2,3 |
2,8 |
2,7 |
2,1 |
1,4 |
3,0 |
2,3 |
3,6 |
2,1 |
2,9 |
a |
| 2022 Mar |
1,9 |
2,7 |
2,7 |
2,0 |
1,4 |
3,1 |
2,2 |
3,7 |
2,2 |
2,6 |
a |
| Dental specialists per 100 000 population |
2020 Mar |
0,3 |
0,0 |
0,0 |
1,0 |
|
0,0 |
0,0 |
0,1 |
|
0,6 |
a |
| 2021 Mar |
0,3 |
0,0 |
0,0 |
0,7 |
0,0 |
0,1 |
0,0 |
0,1 |
|
0,5 |
a |
| 2022 Mar |
0,2 |
|
0,0 |
0,7 |
0,0 |
0,1 |
0,0 |
0,1 |
|
0,6 |
a |
| Dental therapists per 100 000 population |
2020 Mar |
0,7 |
0,3 |
0,0 |
0,4 |
1,0 |
2,4 |
0,6 |
2,2 |
0,4 |
0,0 |
a |
| 2021 Mar |
0,7 |
0,3 |
0,0 |
0,4 |
0,9 |
2,3 |
0,7 |
2,2 |
0,4 |
0,0 |
a |
| 2022 Mar |
0,7 |
0,3 |
0,0 |
0,4 |
0,9 |
2,2 |
0,7 |
2,2 |
0,4 |
0,0 |
a |
| Enrolled nurses per 100 000 population |
2020 Mar |
58,6 |
54,8 |
41,2 |
61,0 |
88,0 |
64,1 |
40,0 |
21,9 |
26,6 |
48,8 |
a |
| 2021 Mar |
62,8 |
68,4 |
48,6 |
66,0 |
94,6 |
56,6 |
35,3 |
24,3 |
34,5 |
51,9 |
a |
| 2022 Mar |
61,2 |
57,8 |
48,7 |
63,3 |
96,5 |
55,4 |
36,7 |
22,7 |
32,9 |
52,5 |
a |
| Environmental health practitioners per 100 000 population |
2020 Mar |
1,1 |
0,4 |
2,9 |
1,2 |
0,9 |
1,3 |
1,5 |
2,2 |
1,8 |
|
a |
| 2021 Mar |
1,1 |
0,5 |
2,3 |
1,3 |
0,8 |
1,0 |
1,4 |
1,8 |
2,6 |
|
a |
| 2022 Mar |
0,4 |
0,4 |
4,4 |
1,5 |
0,8 |
1,4 |
1,6 |
3,0 |
3,5 |
|
a |
| Medical practitioners per 100 000 population |
2020 Mar |
33,6 |
34,1 |
27,9 |
33,9 |
39,1 |
24,8 |
27,0 |
37,9 |
28,3 |
41,6 |
a |
| 2021 Mar |
36,5 |
35,7 |
33,3 |
38,3 |
41,7 |
26,0 |
28,9 |
40,9 |
32,9 |
43,7 |
a |
| 2022 Mar |
32,6 |
36,1 |
32,9 |
39,7 |
41,7 |
27,4 |
28,0 |
41,2 |
33,3 |
41,7 |
a |
| Medical researchers per 100 000 population |
2020 Mar |
0,1 |
0,0 |
0,1 |
0,1 |
0,1 |
0,0 |
|
0,1 |
|
0,1 |
a |
| 2021 Mar |
0,1 |
0,0 |
0,1 |
0,1 |
0,1 |
0,0 |
|
0,1 |
|
0,1 |
a |
| 2022 Mar |
0,1 |
0,0 |
|
0,1 |
0,0 |
0,0 |
|
0,1 |
|
0,1 |
a |
| Medical specialists per 100 000 population |
2020 Mar |
9,6 |
3,8 |
12,6 |
15,7 |
8,2 |
1,4 |
1,8 |
4,1 |
4,2 |
22,5 |
a |
| 2021 Mar |
9,3 |
3,8 |
12,5 |
15,1 |
8,3 |
1,5 |
1,5 |
3,8 |
3,8 |
21,4 |
a |
| 2022 Mar |
9,2 |
3,7 |
13,4 |
15,1 |
7,9 |
1,5 |
1,5 |
3,5 |
4,0 |
20,3 |
a |
| Nursing assistants per 100 000 population |
2020 Mar |
66,4 |
89,1 |
80,6 |
54,6 |
57,5 |
82,5 |
36,1 |
75,5 |
76,5 |
75,5 |
a |
| 2021 Mar |
70,8 |
100,9 |
89,4 |
60,9 |
54,9 |
78,9 |
48,6 |
81,0 |
85,4 |
77,8 |
a |
| 2022 Mar |
68,2 |
86,7 |
91,4 |
60,1 |
53,3 |
78,8 |
50,2 |
77,5 |
85,4 |
74,6 |
a |
| Occupational therapists per 100 000 population |
2020 Mar |
2,6 |
2,5 |
3,0 |
2,4 |
1,9 |
3,9 |
2,3 |
5,0 |
1,7 |
2,9 |
a |
| 2021 Mar |
2,8 |
2,8 |
3,1 |
2,8 |
2,1 |
3,7 |
2,6 |
4,9 |
2,3 |
2,9 |
a |
| 2022 Mar |
2,1 |
2,7 |
3,2 |
3,6 |
2,1 |
3,6 |
2,4 |
4,8 |
1,9 |
2,8 |
a |
| Optometrists per 100 000 population |
2020 Mar |
0,5 |
0,1 |
0,2 |
0,5 |
0,6 |
2,0 |
0,2 |
0,2 |
0,1 |
0,0 |
a |
| 2021 Mar |
0,5 |
0,1 |
0,2 |
0,5 |
0,6 |
2,0 |
0,2 |
0,2 |
0,1 |
0,0 |
a |
| 2022 Mar |
0,5 |
0,1 |
0,2 |
0,5 |
0,6 |
1,9 |
0,2 |
0,2 |
0,1 |
0,0 |
a |
| Pharmacists per 100 000 population |
2020 Mar |
11,8 |
15,4 |
14,4 |
10,7 |
9,3 |
10,5 |
8,6 |
13,1 |
9,5 |
18,4 |
a |
| 2021 Mar |
12,1 |
16,2 |
15,1 |
11,1 |
9,4 |
10,4 |
9,2 |
14,5 |
9,8 |
18,2 |
a |
| 2022 Mar |
11,1 |
15,8 |
18,9 |
11,0 |
9,6 |
11,5 |
9,6 |
12,6 |
9,4 |
18,5 |
a |
| Physiotherapists per 100 000 population |
2020 Mar |
2,9 |
3,0 |
3,1 |
2,4 |
3,1 |
3,0 |
2,7 |
5,1 |
2,8 |
3,0 |
a |
| 2021 Mar |
3,2 |
3,2 |
3,2 |
2,8 |
3,4 |
3,1 |
2,7 |
5,4 |
3,3 |
3,2 |
a |
| 2022 Mar |
2,4 |
3,3 |
3,0 |
2,2 |
3,5 |
3,2 |
2,5 |
5,1 |
2,9 |
3,2 |
a |
| Professional nurses per 100 000 population |
2020 Mar |
145,4 |
193,8 |
88,7 |
124,1 |
169,8 |
164,5 |
149,9 |
146,1 |
142,9 |
100,0 |
a |
| 2021 Mar |
153,6 |
194,0 |
102,3 |
136,4 |
184,1 |
163,4 |
155,6 |
152,1 |
153,8 |
106,0 |
a |
| 2022 Mar |
146,9 |
190,6 |
112,7 |
138,4 |
186,2 |
159,0 |
154,6 |
140,9 |
152,8 |
102,7 |
a |
| Psychologists per 100 000 population |
2020 Mar |
1,4 |
1,2 |
1,2 |
2,0 |
0,7 |
2,2 |
0,8 |
1,5 |
1,3 |
1,6 |
a |
| 2021 Mar |
1,5 |
1,2 |
1,3 |
2,1 |
0,8 |
2,1 |
1,2 |
1,5 |
1,5 |
1,5 |
a |
| 2022 Mar |
1,5 |
1,1 |
1,2 |
2,2 |
1,0 |
2,4 |
1,2 |
1,6 |
1,4 |
1,9 |
a |
| Radiographers per 100 000 population |
2020 Mar |
6,1 |
6,7 |
6,5 |
6,3 |
6,7 |
4,0 |
3,7 |
8,1 |
4,1 |
8,5 |
a |
| 2021 Mar |
6,3 |
7,0 |
6,9 |
7,0 |
6,8 |
3,9 |
3,8 |
8,5 |
4,1 |
8,6 |
a |
| 2022 Mar |
5,7 |
6,6 |
7,0 |
8,0 |
6,6 |
3,6 |
3,7 |
7,8 |
4,2 |
8,4 |
a |
| Speech therapists and audiologists per 100 000 population |
2020 Mar |
1,5 |
1,1 |
0,7 |
1,6 |
1,6 |
1,4 |
1,9 |
2,3 |
1,3 |
1,4 |
a |
| 2021 Mar |
1,7 |
1,2 |
0,8 |
1,9 |
2,1 |
1,4 |
2,0 |
2,6 |
1,5 |
1,4 |
a |
| 2022 Mar |
1,2 |
1,2 |
1,0 |
1,5 |
2,2 |
1,4 |
1,9 |
2,6 |
1,7 |
1,4 |
a |
| Student nurses per 100 000 population |
2020 Mar |
5,5 |
|
|
13,5 |
4,5 |
2,8 |
13,5 |
|
0,2 |
|
a |
| 2021 Mar |
3,3 |
|
|
5,7 |
4,6 |
2,4 |
10,0 |
|
0,0 |
|
a |
| 2022 Mar |
1,9 |
|
|
0,3 |
5,2 |
0,3 |
8,7 |
|
0,1 |
|
a |
Reference notes
a PERSAL.104
b World Health Statistics 2022.32
Definitions
- Indicators are calculated as the number of the specified cadre of health professional per 100 000 uninsured population, as calculated using the webDHIS 2000-30 population time series and the Insight Actuaries modelled estimates for medical schemes coverage at district level circa 2018.
Lack of human resources for health remains a constant feature of many health systems, even in more well-resourced settings. A Global Burden of Disease (GBD) 2019 mapping exercise set targets of 20.7 physicians per 10 000 population, 70.6 nurses and midwives, 8.2 dentistry personnel, and 9.4 pharmaceutical personnel, in order to reach a universal health coverage index of 80 out of 100.105 On this basis, the 2019 global health workforce was estimated to be missing 6.4 million physicians, 30.6 million nurses and midwives, 3.3 million dentistry personnel, and 2.9 million pharmaceutical personnel. Not surprisingly, the lowest health worker densities were recorded in sub-Saharan Africa, south Asia, North Africa and the Middle East. There was a noticeable increase in the medical doctors professional nurses, enrolled nurses, nursing assistants and pharmacists per 100 000 uninsured population between March 2020 and March 2021 as more professionals were appointed to work during the COVID-19 pandemic. The numbers, however, declined in March 2022 to be in line with March 2020 levels.
6.3. Health financing
As shown in Table 21, medical scheme coverage has continued to decline as a percentage of the total population. The Council for Medical Schemes’ 2021 Industry Report noted a further minor consolidation in the number of medical schemes.19 In 2021, there were 75 registered medical schemes, of which 57 were restricted and 18 open. This was almost half the number of schemes operating in the year 2000 (144 schemes, 97 restricted, 47 open). In 2021, the medical schemes disbursed a total of R205.3 billion in benefits, representing a 15.3% increase from 2020. The average amount paid per beneficiary per annum was R23 060.79. Although it is difficult to compare the expenditure patterns with those ordinarily reported for the public sector (as shown in Table 21), the following headline amounts are striking: medical schemes spent 35.7% of their overall disbursements (from risk and savings) on hospital services, 28.1% on specialists, and 16.1% on medicine dispensed outside of hospitals (by pharmacies and dispensing practitioners). Total hospital expenditure increased by 18.7% between 2020 and 2021 as illustrated in Table 22, with almost all benefits (92%) being paid to private hospitals. Year-on-year, medicines expenditure outside of hospitals increased by 9.2%. In the public sector, normalised expenditure on primary health care and district health services expenditure was distinctly higher in 2020/21 in real terms compared with the previous and following financial years; expenditure per headcount increased by almost 50% nationally in 2020/21. This was the result of the drop of the PHC headcount from almost 120 million in 2019/20 to 95 million in 2020/21 and also the drops in the BUR/OPD headcount and PDE in those periods (Figure 41 and Table 23).
Table 21.Trends in overall provincial and local government health expenditure by programme (Rand million, nominal prices), 2012/13 - 2021/22
| Rand million |
Financial Year |
| Prog |
FY 2013 |
FY 2014 |
FY 2015 |
FY 2016 |
FY 2017 |
FY 2018 |
FY 2019 |
FY 2020 |
FY 2021 |
FY 2022 |
| 1. Administration |
3 019 |
3 578 |
3 599 |
4 313 |
4 462 |
4 690 |
5 129 |
5 368 |
8 799 |
7 596 |
| 2. District Health Services |
53 586 |
57 991 |
64 181 |
69 854 |
76 540 |
83 671 |
90 978 |
98 688 |
109 448 |
115 084 |
| 3. Emergency Health Services |
5 079 |
5 352 |
5 556 |
6 025 |
6 435 |
7 380 |
7 671 |
8 394 |
8 660 |
8 791 |
| 4. Provincial Hospital Services |
27 741 |
26 420 |
28 694 |
29 576 |
29 675 |
32 262 |
34 275 |
36 609 |
37 623 |
39 134 |
| 5. Central Hospital Services |
18 822 |
23 559 |
25 804 |
29 529 |
33 736 |
37 437 |
41 120 |
44 608 |
47 516 |
47 227 |
| 6. Health Sciences and Training |
3 755 |
4 039 |
4 248 |
4 529 |
5 107 |
4 916 |
5 037 |
5 115 |
4 796 |
4 792 |
| 7. Health Care Support Services |
1 640 |
1 877 |
1 322 |
2 834 |
1 796 |
1 806 |
4 661 |
2 301 |
3 469 |
3 073 |
| 8. Health Facilities Management |
8 967 |
7 895 |
7 491 |
8 514 |
8 316 |
8 651 |
9 014 |
9 844 |
11 526 |
10 433 |
| Local government expenditure |
2 859 |
2 869 |
3 389 |
3 730 |
4 103 |
4 199 |
4 858 |
4 828 |
5 392 |
5 158 |
| Other |
4 |
|
- |
|
|
- |
- |
- |
- |
- 14 |
| Grand Total |
125 473 |
133 581 |
144 283 |
158 903 |
170 171 |
185 013 |
202 744 |
215 755 |
237 229 |
241 273 |
Source: National Treasury databases.106
Note: ‘Other’ includes any other expenditure not indicated as being allocated to any of the above budget programmes.
Table 22.Provincial and local government health expenditure per province by programme (Rand million), 2021/22
| Rand million |
Financial Year 2021/22 |
| Programme |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
| 1. Administration |
7 596 |
770 |
324 |
2 173 |
1 040 |
285 |
421 |
260 |
907 |
1 414 |
| 2. District Health Services |
115 084 |
15 109 |
5 834 |
19 251 |
27 363 |
14 488 |
10 347 |
2 828 |
8 216 |
11 647 |
| 3. Emergency Health Services |
8 791 |
1 354 |
960 |
1 432 |
1 597 |
904 |
422 |
407 |
475 |
1 240 |
| 4. Provincial Hospital Services |
39 134 |
3 740 |
1 665 |
10 697 |
11 801 |
2 771 |
1 643 |
470 |
2 076 |
4 270 |
| 5. Central Hospital Services |
47 227 |
4 698 |
2 477 |
20 332 |
5 355 |
2 108 |
1 438 |
1 212 |
2 106 |
7 501 |
| 6. Health Sciences and Training |
4 792 |
775 |
261 |
707 |
1 362 |
499 |
409 |
153 |
282 |
344 |
| 7. Health Care Support Services |
3 073 |
113 |
157 |
389 |
169 |
569 |
240 |
175 |
714 |
546 |
| 8. Health Facilities Management |
10 433 |
1 088 |
534 |
2 068 |
1 942 |
1 285 |
1 567 |
380 |
610 |
959 |
| Local government expenditure |
5 158 |
245 |
47 |
2 801 |
538 |
89 |
111 |
34 |
55 |
1 238 |
| Total |
241 287 |
27 891 |
12 260 |
59 850 |
51 168 |
22 999 |
16 598 |
5 921 |
15 442 |
29 160 |
Source: National Treasury databases.106

Figure 41.Percentage of expenditure per programme by province, 2020/21 compared to 2021/22
Source: National Treasury databases.106
Table 23.Health financing indicators by province, 2019 - 2022
| Indicator |
Period |
Sex|Age|Series|Cat |
SA |
EC |
FS |
GP |
KZ |
LP |
MP |
NC |
NW |
WC |
Ref |
| Claims ratio |
2019 |
both sexes all ages med schemes |
90,6 |
|
|
|
|
|
|
|
|
|
a |
| 2020 |
both sexes all ages med schemes |
81,4 |
|
|
|
|
|
|
|
|
|
b |
| 2021 |
both sexes all ages med schemes |
90,9 |
|
|
|
|
|
|
|
|
|
c |
| Expenditure per patient day equivalent (district hospitals) |
2019/20 |
BAS real 2021/22 prices |
3 319 |
3 324 |
3 174 |
3 807 |
3 373 |
3 491 |
3 040 |
3 352 |
3 832 |
2 805 |
d |
| 2020/21 |
BAS real 2021/22 prices |
4 017 |
4 388 |
3 492 |
4 776 |
4 145 |
3 984 |
3 592 |
4 170 |
4 324 |
3 347 |
d |
| 2021/22 |
BAS real 2021/22 prices |
3 450 |
2 730 |
3 194 |
4 250 |
3 903 |
3 725 |
3 325 |
3 756 |
3 840 |
2 884 |
d |
| Medical scheme beneficiaries |
2019 |
both sexes med schemes |
8 990 106 |
653 755 |
390 841 |
3 598 421 |
1 265 694 |
460 369 |
550 360 |
177 151 |
476 557 |
1 333 363 |
a |
| 2020 |
both sexes all ages med schemes |
8 895 152 |
664 509 |
396 758 |
3 436 286 |
1 290 329 |
456 321 |
555 404 |
181 845 |
472 351 |
1 387 206 |
c |
| 2021 |
both sexes all ages med schemes |
8 938 872 |
660 064 |
400 721 |
3 496 871 |
1 274 134 |
468 362 |
556 393 |
193 501 |
469 846 |
1 384 260 |
c |
| Medical scheme coverage |
2019 |
both sexes all ages GHS |
17,2 |
10,8 |
14,7 |
24,9 |
13,1 |
9,9 |
12,6 |
19,3 |
16,3 |
24,1 |
e |
| both sexes all ages med schemes |
15,1 |
7,0 |
4,0 |
40,0 |
14,0 |
5,0 |
6,0 |
2,0 |
6,0 |
15,0 |
a |
| 2020 |
both sexes all ages med schemes |
14,8 |
7,0 |
4,0 |
39,0 |
15,0 |
5,0 |
6,0 |
2,0 |
5,0 |
16,0 |
b |
| 2021 |
both sexes all ages GHS |
16,1 |
10,6 |
16,3 |
24,0 |
10,5 |
8,2 |
9,1 |
19,6 |
15,3 |
23,7 |
f |
| med schemes |
14,9 |
7,0 |
4,0 |
39,0 |
14,0 |
5,0 |
6,0 |
2,0 |
5,0 |
15,0 |
c |
| Medical scheme coverage (ave) |
2018 |
both sexes all ages GHS model |
15,4 |
9,8 |
13,5 |
24,6 |
11,2 |
7,2 |
12,5 |
15,1 |
11,9 |
20,1 |
g |
| Pensioner ratio |
2019 |
both sexes med schemes |
8,6 |
|
|
|
|
|
|
|
|
|
a |
| female med schemes |
9,5 |
|
|
|
|
|
|
|
|
|
a |
| male med schemes |
7,6 |
|
|
|
|
|
|
|
|
|
a |
| 2020 |
both sexes all ages med schemes |
8,9 |
|
|
|
|
|
|
|
|
|
b |
| 2021 |
both sexes med schemes |
9,0 |
|
|
|
|
|
|
|
|
|
b |
| female med schemes |
10,0 |
|
|
|
|
|
|
|
|
|
c |
| male med schemes |
7,8 |
|
|
|
|
|
|
|
|
|
c |
| Proportion of population with large household expenditures on health as a share of total household expenditure or income |
2010-2018 |
both sexes WHO >10% |
1,4 |
|
|
|
|
|
|
|
|
|
h |
| both sexes WHO >25% |
0,1 |
|
|
|
|
|
|
|
|
|
h |
| 2012-2020 |
both sexes WHO >10% |
1,0 |
|
|
|
|
|
|
|
|
|
i |
| both sexes WHO >25% |
0,1 |
|
|
|
|
|
|
|
|
|
i |
| Provincial & LG District Health Services expenditure per capita (uninsured) |
2019/20 |
BAS real 2021/22 prices |
2 154 |
2 331 |
1 981 |
1 693 |
2 393 |
2 602 |
2 328 |
2 402 |
1 887 |
2 112 |
d |
| 2020/21 |
BAS real 2021/22 prices |
2 228 |
2 530 |
2 278 |
1 773 |
2 462 |
2 542 |
2 252 |
2 366 |
1 986 |
2 206 |
d |
| 2021/22 |
BAS real 2021/22 prices |
2 102 |
2 321 |
2 171 |
1 480 |
2 485 |
2 410 |
2 341 |
2 414 |
2 094 |
1 928 |
d |
| Provincial & LG PHC expenditure per capita (uninsured) |
2019/20 |
BAS real 2021/22 prices |
1 328 |
1 241 |
1 245 |
1 311 |
1 534 |
1 172 |
1 276 |
1 476 |
1 290 |
1 316 |
d |
| 2020/21 |
BAS real 2021/22 prices |
1 407 |
1 361 |
1 585 |
1 372 |
1 668 |
1 193 |
1 252 |
1 466 |
1 223 |
1 410 |
d |
| 2021/22 |
BAS real 2021/22 prices |
1 286 |
1 265 |
1 494 |
1 045 |
1 708 |
1 154 |
1 247 |
1 481 |
1 229 |
1 125 |
d |
| Provincial & LG PHC expenditure per PHC headcount |
2019/20 |
BAS real 2021/22 prices |
552 |
458 |
576 |
707 |
543 |
455 |
558 |
582 |
595 |
503 |
d |
| 2020/21 |
BAS real 2021/22 prices |
745 |
637 |
824 |
953 |
742 |
540 |
700 |
721 |
701 |
821 |
d |
| 2021/22 |
BAS real 2021/22 prices |
648 |
560 |
785 |
676 |
732 |
511 |
670 |
699 |
682 |
583 |
d |
| Total net official development assistance to medical research and basic health sectors per capita (US$), by recipient country |
2018 |
both sexes WHO |
2,6 |
|
|
|
|
|
|
|
|
|
h |
| 2019 |
WHO |
1,9 |
|
|
|
|
|
|
|
|
|
j |
| 2020 |
both sexes WHO |
0,8 |
|
|
|
|
|
|
|
|
|
i |
Reference notes
a Medical Schemes 2019-20.77
b Medical Schemes 2020-21.17
c Medical Schemes 2021-22.19
d National Treasury.106
e Stats SA GHS 2019.16
f Stats SA GHS 2021.18
g Insight Med Schemes 2019.107
h World Health Statistics 2020.78
i World Health Statistics 2022.32
j World Health Statistics 2021.31
Definitions
- Claims ratio [Percentage]: Proportion of member contributions that has been utilised for the payment of benefits claimed by members of medical schemes, as opposed to allocation of contributions for non-health benefits and the building of reserves.
- Expenditure per patient day equivalent (district hospitals) [Rand (real prices)]: Average cost per patient per day seen in a hospital (expressed as Rand per patient day equivalent).
- Medical scheme beneficiaries [Number]: Number of medical scheme beneficiaries, as reported by the Medical Schemes Council.
- Medical scheme coverage (ave) [Percentage]: Percentage of population who have medical scheme insurance.
- Medical scheme coverage [Percentage]: Proportion of population covered by medical schemes.
- Pensioner ratio [Percentage]: Proportion of members of medical schemes who are 65 years or older, in registered medical schemes.
- Proportion of population with large household expenditures on health as a share of total household expenditure or income [Percentage]: Proportion of population (%) with total household expenditures on health >10% and >25% of total household expenditure or income
- Provincial & LG District Health Services expenditure per capita (uninsured) [Rand (real prices)]: Provincial expenditure on District Health Services (all sub-programmes except 2.8 Coroner services) plus net local government expenditure on PHC per uninsured population.
- Provincial & LG PHC expenditure per capita (uninsured) [Rand (real prices)]: Provincial expenditure on sub-programmes of DHS (2.2 - 2.7) plus net local government expenditure on PHC per uninsured population.
- Provincial & LG PHC expenditure per PHC headcount [Rand (real prices)]: Provincial expenditure on sub-programmes of DHS (2.2 - 2.7) plus net local government expenditure on PHC divided by PHC headcount from webDHIS.
7. Conclusion
While the world and South Africa are still in the early post-COVID era, there is already a global (and national) focus on learning lessons from the pandemic in order to build a more resilient health system that can be responsive to unexpected shocks. Strong health-information systems should be the foundation on which evidence-based decisions can be made in order to support strong governance and leadership, where human resources for health are also supported and healthcare funding is prioritised. However, there is also an understandable tendency to revert to the status quo ante to recover lost ground and reinstate systems that were compromised. This is particularly true in a setting of extreme fiscal constraint, where health systems in the public sector are being asked to accept real declines in funding and the private sector continues to face unaffordable increases in medical scheme subscription costs for a stagnant and aging risk pool. Where health-information systems that bridged the divide between the public and private sectors lose funding, the previous fragmentation is re-imposed. Lessons learned risk being lost, despite the lip-service paid to post-pandemic preparedness and response frameworks.